Wellcare Appeal Form 2022
Wellcare Appeal Form 2022 - Submit and review your requests online @ provider.wellcare.com requestor’s name: You can now quickly request an appeal for your drug coverage through the request for redetermination form. Web for a state provider appeal within 120 calendar days from the date of our appeal resolution letter. Web medication appeal request form (pdf) medicaid drug coverage request form (pdf) notice of pregnancy form (pdf) provider incident report form (pdf) pcp change. Complaints should be addressed to: All fields are required information: Web 1 dec 2021 — forms applicable to part d grievances, coverage determinations and exceptions, and appeals processes. If the standard time for making a determination could seriously jeopardize the life and/or health of the member or the member's ability to regain. Ad you may qualify for up to $2,500 in extra dental, vision, or hearing care. This letter will notify you of any adverse benefit determination.
For help on how to ask for a state provider appeal, call the mo healthnet division. Submit and review your requests online @ provider.wellcare.com requestor’s name: Web please wait while your request is being processed. Web 1 dec 2021 — forms applicable to part d grievances, coverage determinations and exceptions, and appeals processes. Complete, sign and mail this request to the address at the end of this form, or fax it to. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Web medication appeal request form (pdf) medicaid drug coverage request form (pdf) notice of pregnancy form (pdf) provider incident report form (pdf) pcp change. Web because we, wellcare, denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for redetermination (appeal) of our. You can now quickly request an appeal for your drug coverage through the request for redetermination form. This letter will notify you of any adverse benefit determination.
Web because we, wellcare, denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for redetermination (appeal) of our. Web pro_100620e state approved 09202011 ©wellcare 2022 hi2wcmweb00620e_0000 providers may seek an appeal within 120 calendar days of claims denial. Save or instantly send your ready. Web for a state provider appeal within 120 calendar days from the date of our appeal resolution letter. If the standard time for making a determination could seriously jeopardize the life and/or health of the member or the member's ability to regain. Providers may file a verbal or written complaint with the missouri care complaints and appeals department. Web medication appeal request form you can use this form to request an appeal when a medication coverage determination request has been denied. Web please wait while your request is being processed. Ad you may qualify for up to $2,500 in extra dental, vision, or hearing care. You can now quickly request an appeal for your drug coverage through the request for redetermination form.

Welcare Medicare Prior Authorization Form For Medication Fill Online
Web medication appeal request form (pdf) medicaid drug coverage request form (pdf) notice of pregnancy form (pdf) provider incident report form (pdf) pcp change. Requesting a 2nd appeal (reconsideration) if you’re not satisfied with the outcome of your first appeal. Web please wait while your request is being processed. Web ©wellcare transplant authorizaion request fax to: Ad you may qualify.

Wellcare prior authorization form Fill out & sign online DocHub
Web please wait while your request is being processed. Web medication appeal request form you can use this form to request an appeal when a medication coverage determination request has been denied. Web because we, wellcare, denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for redetermination (appeal) of our..
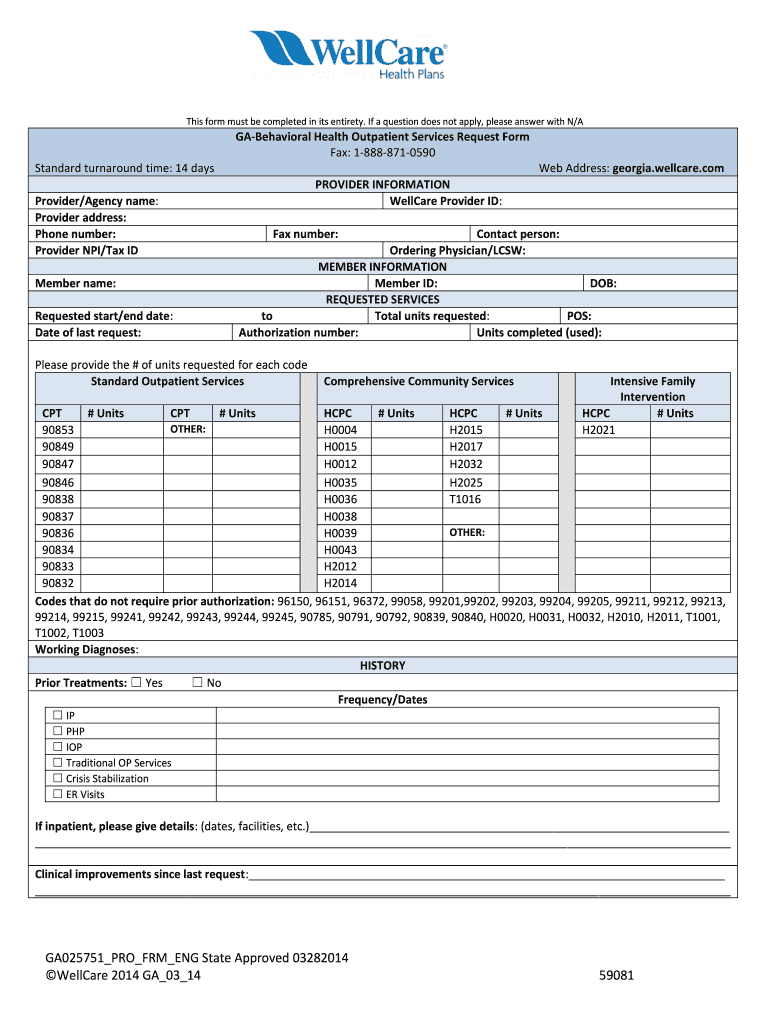
Wellcare Behavioral Health Service Request Form Fill Out and Sign
Web please wait while your request is being processed. Web medication appeal request form you can use this form to request an appeal when a medication coverage determination request has been denied. Providers may file a verbal or written complaint with the missouri care complaints and appeals department. Easily fill out pdf blank, edit, and sign them. Ad you may.

otccatalogMedicareAdvantageMaineoverthecounterCostsorderform
Web for a state provider appeal within 120 calendar days from the date of our appeal resolution letter. Complaints should be addressed to: If the standard time for making a determination could seriously jeopardize the life and/or health of the member or the member's ability to regain. Medicaid members have a right to appeal adverse benefit. Ad you may qualify.
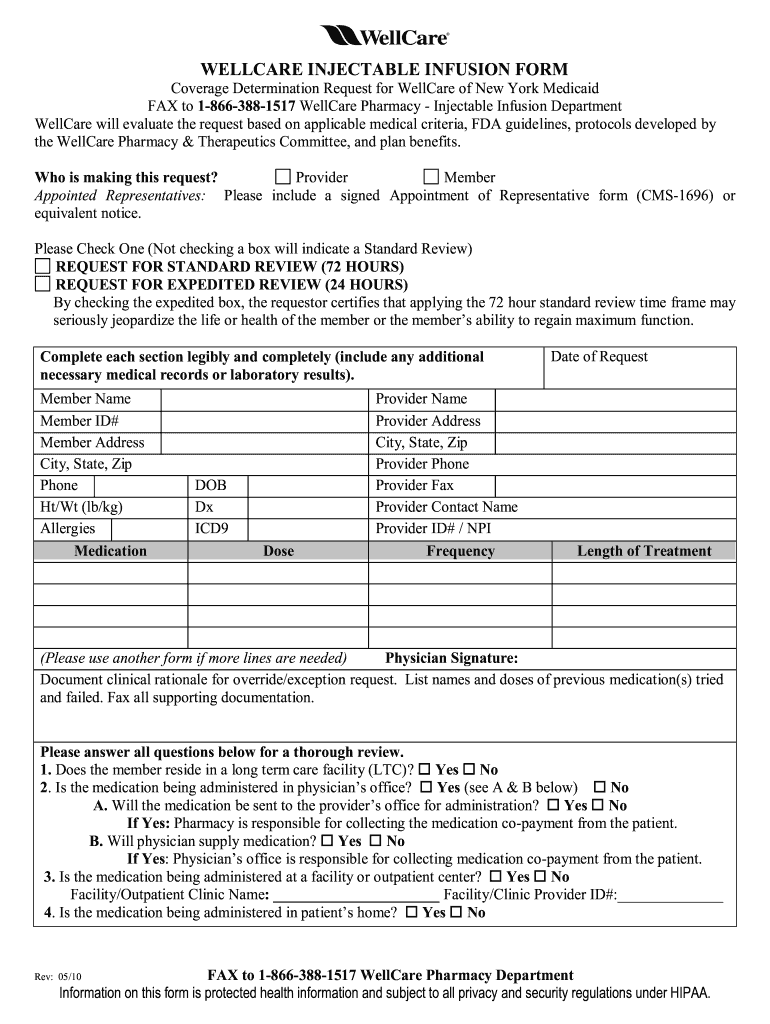
WellCare Injectable Infusion Form 20102022 Fill and Sign Printable
Web pro_100620e state approved 09202011 ©wellcare 2022 hi2wcmweb00620e_0000 providers may seek an appeal within 120 calendar days of claims denial. Requesting a 2nd appeal (reconsideration) if you’re not satisfied with the outcome of your first appeal. Save or instantly send your ready. Wellcare health plans, inc., complies with applicable federal civil rights laws and does not discriminate on the. Web.
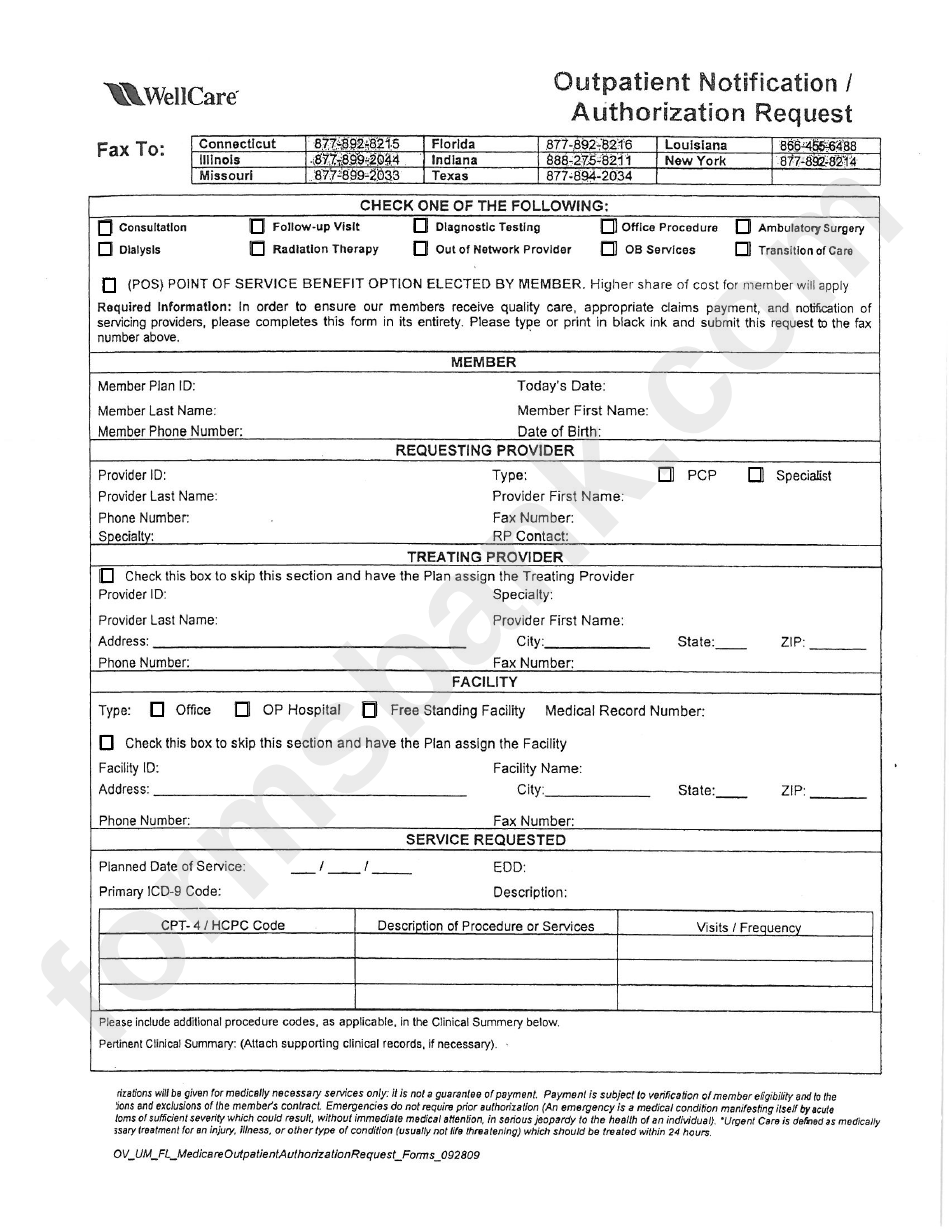
Fillable Outpatient Notification /authorization Request Wellcare
Submit and review your requests online @ provider.wellcare.com requestor’s name: Providers may file a verbal or written complaint with the missouri care complaints and appeals department. Medicaid members have a right to appeal adverse benefit. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Web medication appeal request form you can.
Coverage Area
Complaints should be addressed to: All fields are required information: This letter will notify you of any adverse benefit determination. Web please wait while your request is being processed. Save or instantly send your ready.
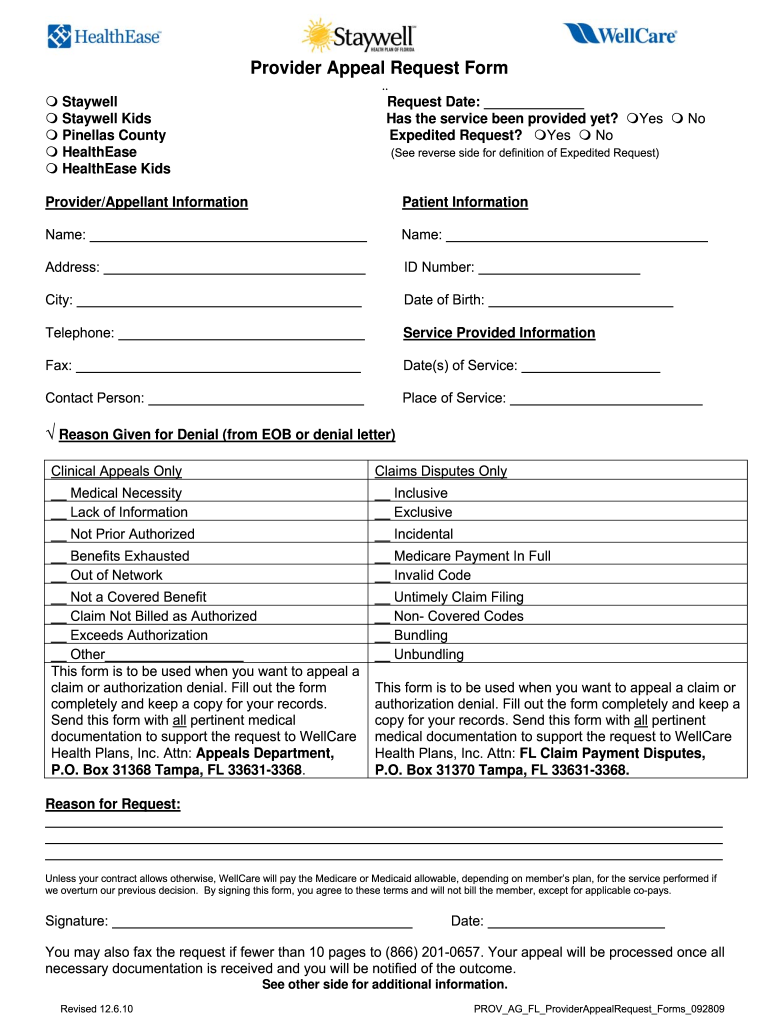
Wellcare Appeal Form Pdf Fill Online, Printable, Fillable, Blank
Submit and review your requests online @ provider.wellcare.com requestor’s name: Medicaid members have a right to appeal adverse benefit. We're here to help you find a plan that fits your needs and budget. This letter will notify you of any adverse benefit determination. Providers may file a verbal or written complaint with the missouri care complaints and appeals department.
WELLCARE HEALTH PLANS, INC. FORM 8K EX99.2 PRESENTATION DATED
Web ©wellcare transplant authorizaion request fax to: Web pro_100620e state approved 09202011 ©wellcare 2022 hi2wcmweb00620e_0000 providers may seek an appeal within 120 calendar days of claims denial. You can now quickly request an appeal for your drug coverage through the request for redetermination form. This letter will notify you of any adverse benefit determination. Web use this form as part.

OvertheCounter (OTC) Catalog WellCare Fill and Sign Printable
Requesting a 2nd appeal (reconsideration) if you’re not satisfied with the outcome of your first appeal. Medicaid members have a right to appeal adverse benefit. Providers may file a verbal or written complaint with the missouri care complaints and appeals department. You can now quickly request an appeal for your drug coverage through the request for redetermination form. Web a.
Web Because We, Wellcare, Denied Your Request For Coverage Of (Or Payment For) A Prescription Drug, You Have The Right To Ask Us For Redetermination (Appeal) Of Our.
Providers may file a verbal or written complaint with the missouri care complaints and appeals department. Easily fill out pdf blank, edit, and sign them. Web medication appeal request form (pdf) medicaid drug coverage request form (pdf) notice of pregnancy form (pdf) provider incident report form (pdf) pcp change. For help on how to ask for a state provider appeal, call the mo healthnet division.
Web You Will Receive A Letter From Wellcare Of North Carolina.
Wellcare health plans, inc., complies with applicable federal civil rights laws and does not discriminate on the. Complete, sign and mail this request to the address at the end of this form, or fax it to. Submit and review your requests online @ provider.wellcare.com requestor’s name: Medicaid members have a right to appeal adverse benefit.
Web Medication Appeal Request Form You Can Use This Form To Request An Appeal When A Medication Coverage Determination Request Has Been Denied.
We have redesigned our website. Ad you may qualify for up to $2,500 in extra dental, vision, or hearing care. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. >>complete your attestation today!<< access key forms.
Web A Member May Designate In Writing To Ambetter That A Provider Is Acting On Behalf Of The Member Regarding The Complaint/Grievance And Appeal Process.
This letter will notify you of any adverse benefit determination. We're here to help you find a plan that fits your needs and budget. Complaints should be addressed to: You can now quickly request an appeal for your drug coverage through the request for redetermination form.