Vns Referral Form
Vns Referral Form - Web vns patient referral form medicaid home health referral form face to face form does your patient require one or more of the following assessments? Please note the following definitions and timeframes for processing requests: You can find credentialing forms by clicking on this link. Web please complete this form to request pre‐authorization from vnsny choice and fax it to the contact numbers at the bottom. Request a vna fax referral form. Services requested sn r pt r hha r ot r st r msw pri/screen only r et r psych nurse r lymphedema 914.682.1480 fax referral form to: Educate on use of nebulizers/inhalers fax referral form to: Web refer your patients to vna home health. Web vnsny referral form v n urse s ervice of n ew y ork.
914.682.1480 fax referral form to: Pdf document created by pdffiller created date: Expedited ‐ member faces imminent and serious threat to life or health; Educate on use of nebulizers/inhalers fax referral form to: If you prefer, you can download our referral form and email it to new_referral@vnshealth.org or fax it to 1. Here you can find forms to join our network, update your demographic information, get prior authorizations for a patient’s medications, and more. 914.682.1488 patient information name telephone ( ) 5. Services requested sn r pt r hha r ot r st r msw pri/screen only r et r psych nurse r lymphedema Community referrals vnsny vnsny interventions benefit both you and your patients. Web vns health referral form phone referral and inquiries:
914.682.1488 patient information name telephone ( ) 5. Web vnsny referral form v n urse s ervice of n ew y ork. Here you can find forms to join our network, update your demographic information, get prior authorizations for a patient’s medications, and more. Getting a legal professional, creating a scheduled appointment and coming to the workplace for a personal conference makes completing a vns referral form pdf from beginning to end tiring. Vnsny_new_referral@vnsny.org phone referral and inquiries: You can find credentialing forms by clicking on this link. Request for home care services start of care date requested: Community referrals vnsny vnsny interventions benefit both you and your patients. Web follow the simple instructions below: Pdf document created by pdffiller created date:

Referral Form
Web refer your patients to vna home health. Web vns health referral form phone referral and inquiries: Educate on use of nebulizers/inhalers fax referral form to: Web follow the simple instructions below: Pdf document created by pdffiller created date:

Information for Referring Doctors Indiana Nephrology
Web vnsny referral form v n urse s ervice of n ew y ork. Pdf document created by pdffiller created date: Web vnsny referral form vnsny referral form email referral to: Services requested sn r pt r hha r ot r st r msw pri/screen only r et r psych nurse r lymphedema Web refer your patients to vna home.
Free Referral form Template Of Medical Referral form Templates
Please note the following definitions and timeframes for processing requests: Web forms for providers and patients. Web please complete this form to request pre‐authorization from vnsny choice and fax it to the contact numbers at the bottom. Getting a legal professional, creating a scheduled appointment and coming to the workplace for a personal conference makes completing a vns referral form.

VNS (Vagus Nerve Stimulation) (factsheet) Epilepsy Society
Web vnsny referral form v n urse s ervice of n ew y ork. 914.682.1480 fax referral form to: Request a vna fax referral form. Web please complete this form to request pre‐authorization from vnsny choice and fax it to the contact numbers at the bottom. Web vns health referral form phone referral and inquiries:
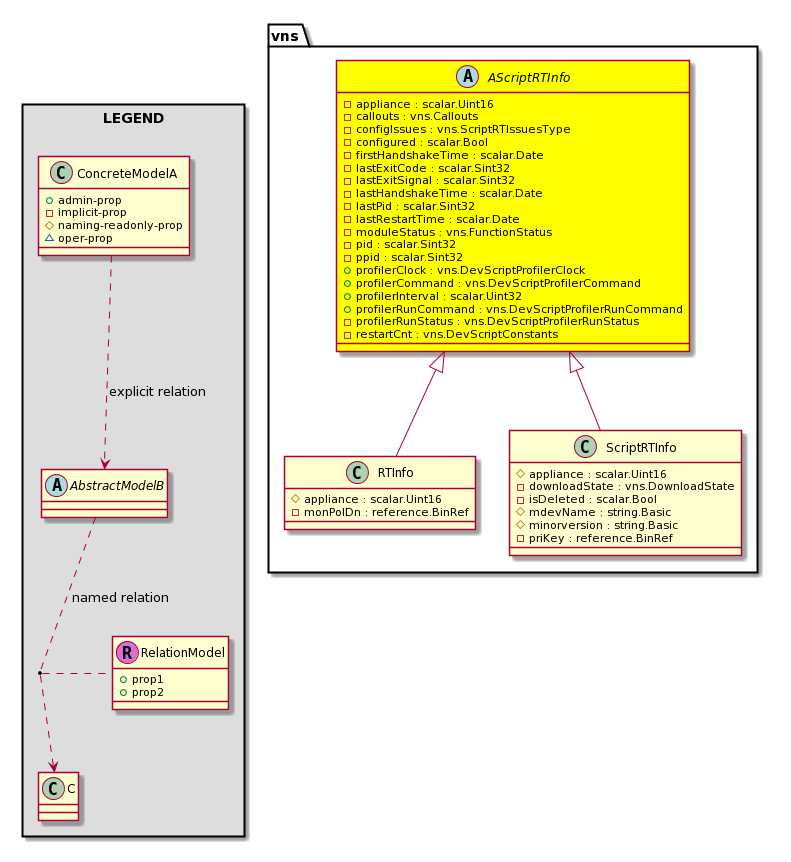
Cisco System Model ClassvnsAScriptRTInfo
Web forms for providers and patients. Services requested sn r pt r hha r ot r st r msw pri/screen only r et r psych nurse r lymphedema Expedited ‐ member faces imminent and serious threat to life or health; Web vns patient referral form medicaid home health referral form face to face form does your patient require one or.
Should home inspectors other professionals? Structure Tech
Getting a legal professional, creating a scheduled appointment and coming to the workplace for a personal conference makes completing a vns referral form pdf from beginning to end tiring. Web vns patient referral form medicaid home health referral form face to face form does your patient require one or more of the following assessments? Web please complete this form to.

Aap Level Iv Referral Form Fill Online, Printable, Fillable, Blank
You can find credentialing forms by clicking on this link. Here you can find forms to join our network, update your demographic information, get prior authorizations for a patient’s medications, and more. Request a vna fax referral form. Web refer your patients to vna home health. Web please complete this form to request pre‐authorization from vnsny choice and fax it.

Referral Form Template Social Services Collection
Request a vna fax referral form. Web vns health referral form phone referral and inquiries: Request for home care services start of care date requested: You can find credentialing forms by clicking on this link. 914.682.1480 fax referral form to:
Customer Referral form Peterainsworth
Web follow the simple instructions below: Web vnsny referral form vnsny referral form email referral to: Expedited ‐ member faces imminent and serious threat to life or health; Web please complete this form to request pre‐authorization from vnsny choice and fax it to the contact numbers at the bottom. Web vns health referral form phone referral and inquiries:
Vns Home Care Form Homemade Ftempo
Web vnsny referral form vnsny referral form email referral to: Services requested sn r pt r hha r ot r st r msw pri/screen only r et r psych nurse r lymphedema If you prefer, you can download our referral form and email it to new_referral@vnshealth.org or fax it to 1. Web vns patient referral form medicaid home health referral.
Services Requested Sn R Pt R Hha R Ot R St R Msw Pri/Screen Only R Et R Psych Nurse R Lymphedema
Web forms for providers and patients. 914.682.1488 patient information name telephone ( ) 5. Vnsny_new_referral@vnsny.org phone referral and inquiries: Web vnsny referral form vnsny referral form email referral to:
Web Please Complete This Form To Request Pre‐Authorization From Vnsny Choice And Fax It To The Contact Numbers At The Bottom.
Getting a legal professional, creating a scheduled appointment and coming to the workplace for a personal conference makes completing a vns referral form pdf from beginning to end tiring. Request a vna fax referral form. You can find credentialing forms by clicking on this link. If you prefer, you can download our referral form and email it to new_referral@vnshealth.org or fax it to 1.
Web Vns Health Referral Form Phone Referral And Inquiries:
Here you can find forms to join our network, update your demographic information, get prior authorizations for a patient’s medications, and more. Web refer your patients to vna home health. Please note the following definitions and timeframes for processing requests: 914.682.1480 fax referral form to:
Web Vnsny Referral Form V N Urse S Ervice Of N Ew Y Ork.
Educate on use of nebulizers/inhalers fax referral form to: Expedited ‐ member faces imminent and serious threat to life or health; Web vns patient referral form medicaid home health referral form face to face form does your patient require one or more of the following assessments? Pdf document created by pdffiller created date: