Transfer Of Medical Records Form
Transfer Of Medical Records Form - Web how to transfer your health records between doctors ask your new doctor if they follow a certain process. Web ideally, the process of requesting for the release or transfer or medical records goes like this: Web updated may 15, 2022 | legally reviewed by susan chai, esq. This form, also known as a medical release form, ensures that your patient information, medical history, and other relevant health records are securely transferred and disclosed. The first article of this authorization requires full identification of the patient executing it. Specify on the form what kind and type of information and records the. Check if you can download your medical records from a patient portal. The federal health insurance portability and accountability act of 1996 (hipaa) and state laws mandate that. You have a new doctor or change doctors. Fill up a medical record transfer form that allows for a medical provider the permission to share the patient’s.
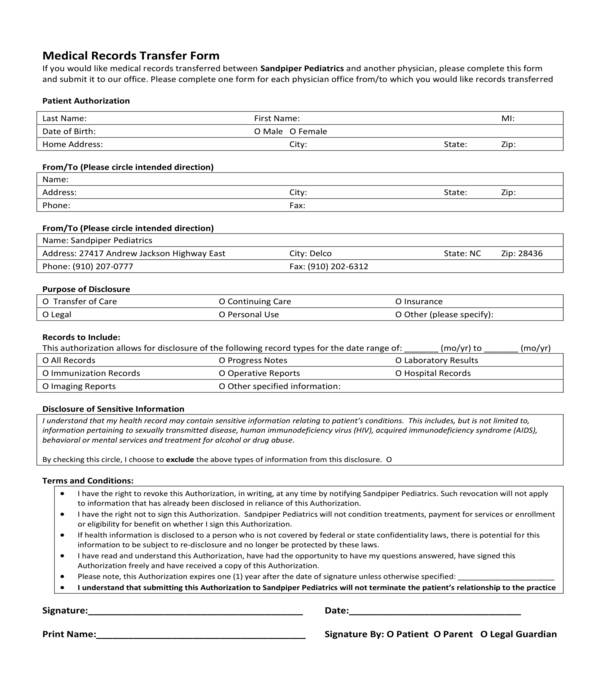
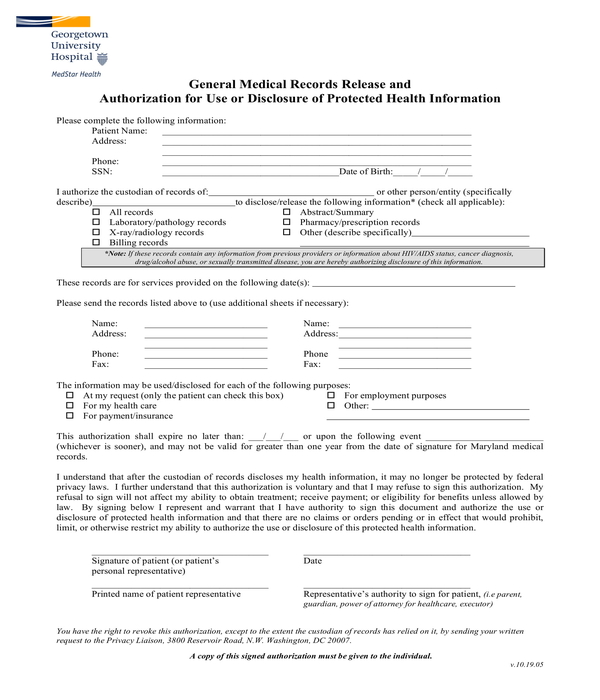
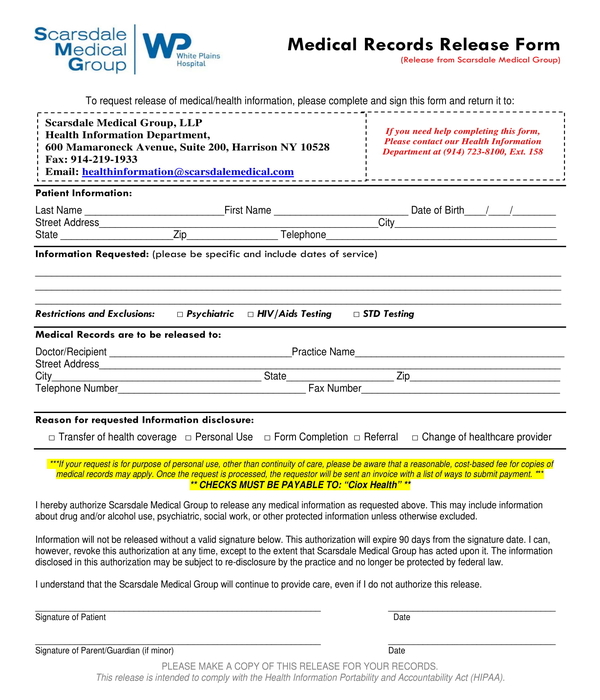
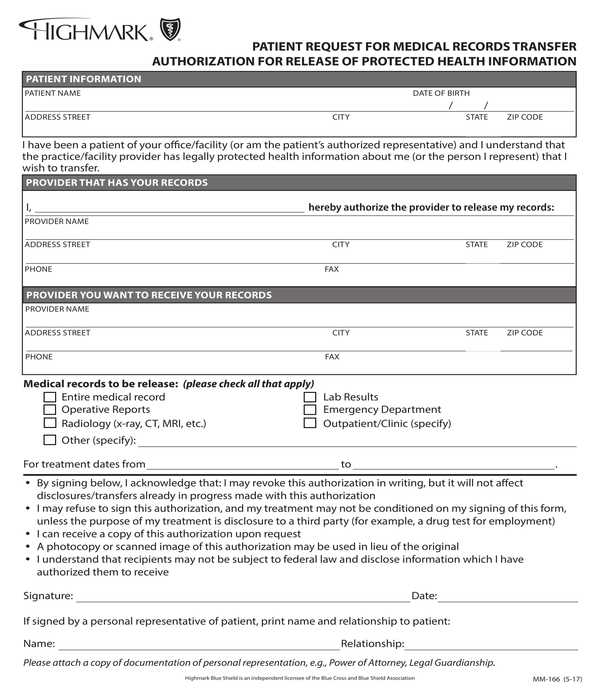
A medical records release (hipaa) form is a written authorization for health providers to release information to the patient as well as someone other than the patient. (name of patient) patient information: If you're a mayo clinic health system patient or have been one in the past, you can use these forms to grant permission for others to access your protected health information or request a change to your health record. You have a new doctor or change doctors. Start by asking questions of your new provider. The first article of this authorization requires full identification of the patient executing it. Use these forms when requesting transfer of your medical and billing records to or from another provider or to obtain a copy of your records: Web the main purpose of a medical records transfer form is to give permission to your current health care provider to release your medical records to a new provider. Check if you can download your medical records from a patient portal. Web this document provides a form for you to authorize the transfer of medical records from one health care provider to another.
A medical records release (hipaa) form is a written authorization for health providers to release information to the patient as well as someone other than the patient. Do you have access to a patient portal from your. Use these forms when requesting transfer of your medical and billing records to or from another provider or to obtain a copy of your records: If you're a mayo clinic health system patient or have been one in the past, you can use these forms to grant permission for others to access your protected health information or request a change to your health record. Download the release of protected health information form. The date when this paperwork should be considered completed with information must be. You have a new doctor or change doctors. In addition to his or her name, the “date of. (name of patient) patient information: Web this document provides a form for you to authorize the transfer of medical records from one health care provider to another.
FREE 11+ Medical Records Transfer Forms in PDF MS Word
The federal health insurance portability and accountability act of 1996 (hipaa) and state laws mandate that. Start by asking questions of your new provider. Web this document provides a form for you to authorize the transfer of medical records from one health care provider to another. In addition to his or her name, the “date of. This form, also known.
FREE 11+ Medical Records Transfer Forms in PDF MS Word
Use these forms when requesting transfer of your medical and billing records to or from another provider or to obtain a copy of your records: Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Web ideally, the process of requesting for the release or.
FREE 11+ Medical Records Transfer Forms in PDF MS Word
A medical records release (hipaa) form is a written authorization for health providers to release information to the patient as well as someone other than the patient. Do you have access to a patient portal from your. If you're a mayo clinic health system patient or have been one in the past, you can use these forms to grant permission.
FREE 12+ Sample Transfer Request Forms in MS Word PDF
This form, also known as a medical release form, ensures that your patient information, medical history, and other relevant health records are securely transferred and disclosed. Web medical and billing record release forms. If you're a mayo clinic health system patient or have been one in the past, you can use these forms to grant permission for others to access.
FREE 11+ Medical Records Transfer Forms in PDF MS Word
Fill up a medical record transfer form that allows for a medical provider the permission to share the patient’s. The federal health insurance portability and accountability act of 1996 (hipaa) and state laws mandate that. Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record..
FREE 11+ Medical Records Transfer Forms in PDF MS Word
Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. The date when this paperwork should be considered completed with information must be. Download the release of protected health information form. A medical records release (hipaa) form is a written authorization for health providers to.
FREE 11+ Medical Records Transfer Forms in PDF MS Word
Web you can still request your medical records or transfer your records from a previous provider to ahn by filling out a form. Start by asking questions of your new provider. Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Specify on the form.
FREE 11+ Medical Records Transfer Forms in PDF MS Word
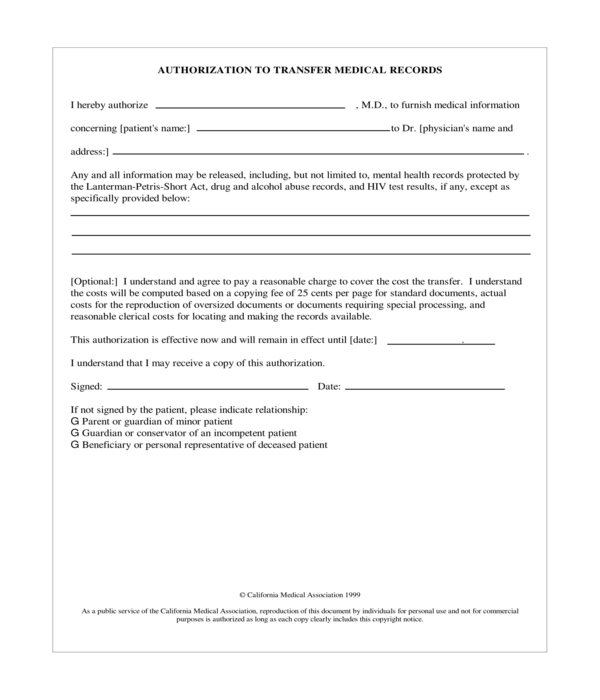
The first article of this authorization requires full identification of the patient executing it. The date when this paperwork should be considered completed with information must be. The federal health insurance portability and accountability act of 1996 (hipaa) and state laws mandate that. A medical records release (hipaa) form is a written authorization for health providers to release information to.
FREE 22+ Medical Consent Forms in PDF Ms Word
If you're a mayo clinic health system patient or have been one in the past, you can use these forms to grant permission for others to access your protected health information or request a change to your health record. Web medical and billing record release forms. Use these forms when requesting transfer of your medical and billing records to or.
FREE 11+ Medical Records Transfer Forms in PDF MS Word
Web the main purpose of a medical records transfer form is to give permission to your current health care provider to release your medical records to a new provider. The first article of this authorization requires full identification of the patient executing it. Web ideally, the process of requesting for the release or transfer or medical records goes like this:.
Web This Document Provides A Form For You To Authorize The Transfer Of Medical Records From One Health Care Provider To Another.
A medical records release (hipaa) form is a written authorization for health providers to release information to the patient as well as someone other than the patient. Download the release of protected health information form. When to use a medical records transfer form: Web how to transfer your health records between doctors ask your new doctor if they follow a certain process.
The Federal Health Insurance Portability And Accountability Act Of 1996 (Hipaa) And State Laws Mandate That.
This form, also known as a medical release form, ensures that your patient information, medical history, and other relevant health records are securely transferred and disclosed. The first article of this authorization requires full identification of the patient executing it. Check if you can download your medical records from a patient portal. (name of patient) patient information:
Fill Up A Medical Record Transfer Form That Allows For A Medical Provider The Permission To Share The Patient’s.
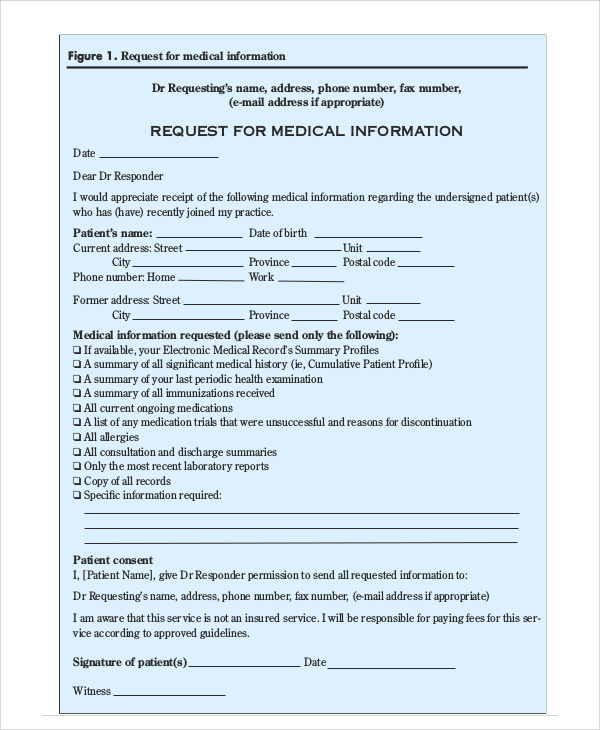
Web ideally, the process of requesting for the release or transfer or medical records goes like this: Web the main purpose of a medical records transfer form is to give permission to your current health care provider to release your medical records to a new provider. Requests should be directed to the facility you were treated at. Web (1) preliminary information.
Do You Have Access To A Patient Portal From Your.
Specify on the form what kind and type of information and records the. You have a new doctor or change doctors. Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. In addition to his or her name, the “date of.