Sutter Health Authorization Form
Sutter Health Authorization Form - Use your zip code to find your personal plan. Use the tools and resources. Web prescription drug prior authorization or step therapy exception request form page 1 of 2 prescription drug prior authorization or. Ad register and subscribe now to work on sutter health radiology images release auth form. Web my health pays rewards® ways to save; Download your adjusted document, export it to the cloud, print it from the editor, or share it with other participants. Web please complete this form if you wish to authorize sutter health plus to disclose your protected health information to another individual or entity. Submit the completed and signed form by: Web authorization for use and disclosure of health information patient name: Web provider forms and resources participating providers:
Download and complete the medical records authorization form. Web prescription drug prior authorization or step therapy exception request form page 1 of 2 prescription drug prior authorization or. Web prescription drug prior authorization or step therapy exception request form page 1 of 2 prescription drug prior authorization or. Submit the completed and signed form by: Complete one authorization for use and. Web authorization for use and disclosure of health information patient name: Sip pcp & specialist rosters. Download your adjusted document, export it to the cloud, print it from the editor, or share it with other participants. Web request by email, fax, mail. Web form to the address or fax number shown on the attached address list for the sutter health affiliate where you received care.
Download and complete the medical records authorization form. Box 211314 eagan, mn 55121 sutter health plus. Emailing the form to mhosupport@sutterhealth.org. Use the tools and resources. Web please complete this form if you wish to authorize sutter health plus to disclose your protected health information to another individual or entity. Web prescription drug prior authorization or step therapy exception request form page 1 of 2 prescription drug prior authorization or. Web provider forms and resources participating providers: Mailing the form to patient services contact center. Web to request your medical record, submit your medical records authorization form online (available in english, spanish or chinese) or sign in to my health online. Complete one authorization for use and.
General Consent Form Sutter Health Fill Out and Sign Printable PDF
Web authorization for use and disclosure of health information patient name: Web fill out an authorization form. Web edit your sutter health release of information online. Web prescription drug prior authorization or step therapy exception request form page 1 of 2 prescription drug prior authorization or. Emailing the form to mhosupport@sutterhealth.org.
11+ Printable Medical Authorization Forms PDF, DOC
Sign it in a few clicks. Commercial hmo claims submission sutter health plus p.o. Use your zip code to find your personal plan. Web how to refer referral documents referral brochure referral intake form interoperability brochure chat with a referral agent our concierge referral team is available to answer. Ad register and subscribe now to work on sutter health radiology.

Gallery of Sutter Health Authorization form Brilliant Authorization
Web provider forms and resources participating providers: Web a my health online account makes managing your care easier. Web prescription drug prior authorization or step therapy exception request form page 1 of 2 prescription drug prior authorization or. Mailing the form to patient services contact center. Web how to refer referral documents referral brochure referral intake form interoperability brochure chat.

Cohere Health Prior Authorization Form Fill and Sign Printable
Sign it in a few clicks. Web rosters and referral forms. Web prescription drug prior authorization or step therapy exception request form page 1 of 2 prescription drug prior authorization or. Submit the completed and signed form by: Type text, add images, blackout confidential details, add comments, highlights and more.
Free Medical Authorization Forms & Templates (Word PDF)
Use the tools and resources. Get the tools you need to easily manage your administrative needs, and your keep your focus on the health of your patients. Download and complete the medical records authorization form. Submit the completed and signed form by: Mailing the form to patient services contact center.
Sutter Health Authorization for Use and Disclosure of Health
Ad register and subscribe now to work on sutter health radiology images release auth form. Web please complete this form if you wish to authorize sutter health plus to disclose your protected health information to another individual or entity. Web provider forms and resources participating providers: Sip pcp & specialist rosters. Box 211314 eagan, mn 55121 sutter health plus.

Sutter Health Form SH0122 20192022 Fill and Sign Printable Template
Type text, add images, blackout confidential details, add comments, highlights and more. Web please complete this form if you wish to authorize sutter health plus to disclose your protected health information to another individual or entity. Web to request your medical record, submit your medical records authorization form online (available in english, spanish or chinese) or sign in to my.
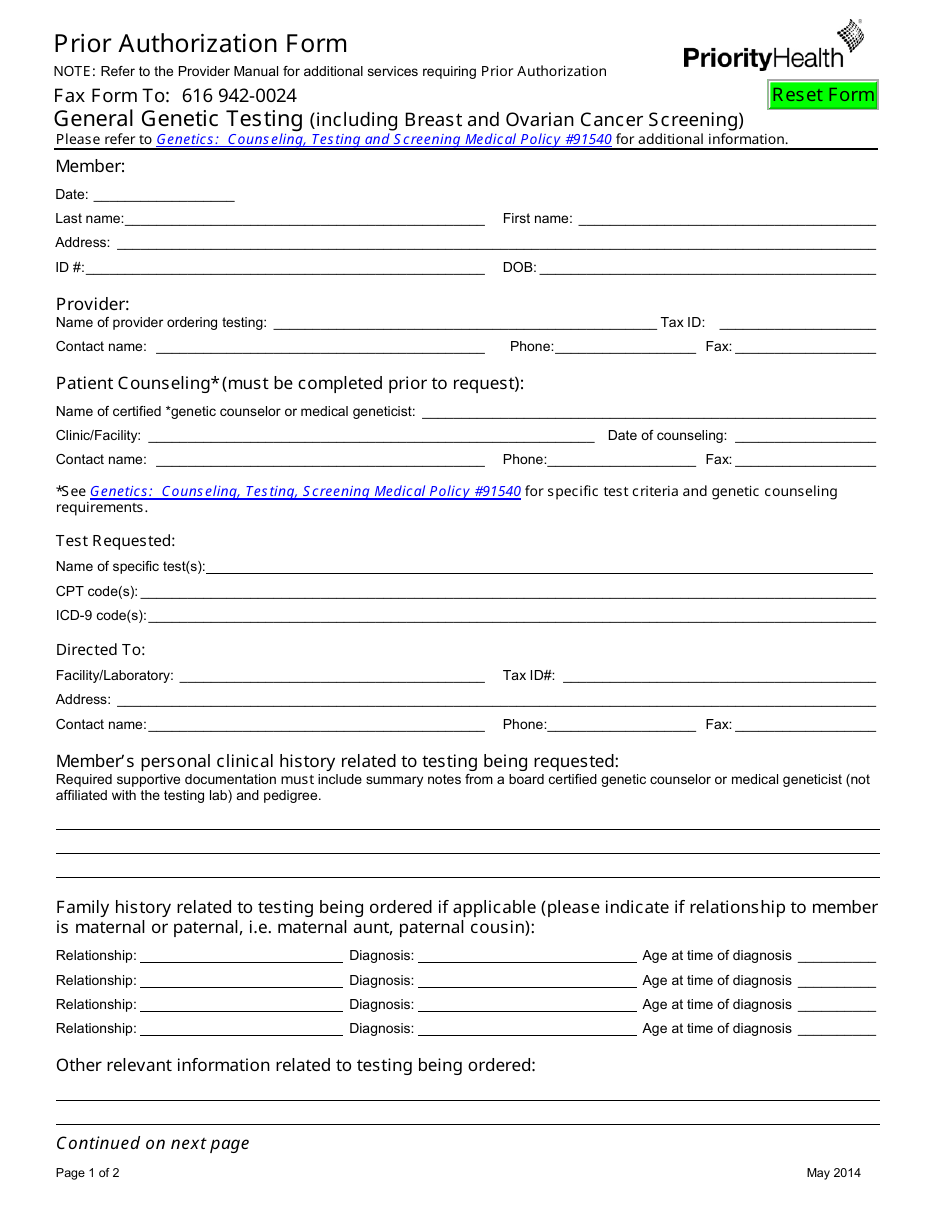
Prior Authorization Form Priorityhealth Download Fillable PDF
Sign it in a few clicks. Web edit your sutter health release of information online. Web your written authorization will typically be required for most uses and disclosures of psychotherapy notes, if you receive treatment in an addiction treatment. Web my health pays rewards® ways to save; Web prescription drug prior authorization or step therapy exception request form page 1.

Sutter Health SEBMF Milvia Street Medical Office Building Berkeley, CA
Web how to refer referral documents referral brochure referral intake form interoperability brochure chat with a referral agent our concierge referral team is available to answer. Sip pcp & specialist rosters. Web to request your medical record, submit your medical records authorization form online (available in english, spanish or chinese) or sign in to my health online. Commercial hmo claims.

ads/responsive.txt Sutter Health Authorization form Brilliant
Web rosters and referral forms. Web provider forms and resources participating providers: Sip pcp & specialist rosters. Web fill out an authorization form. Web prescription drug prior authorization or step therapy exception request form page 1 of 2 prescription drug prior authorization or.
Box 211314 Eagan, Mn 55121 Sutter Health Plus.
Type text, add images, blackout confidential details, add comments, highlights and more. Web form to the address or fax number shown on the attached address list for the sutter health affiliate where you received care. Web provider forms and resources participating providers: Mailing the form to patient services contact center.
Web How To Refer Referral Documents Referral Brochure Referral Intake Form Interoperability Brochure Chat With A Referral Agent Our Concierge Referral Team Is Available To Answer.
Web prescription drug prior authorization or step therapy exception request form page 1 of 2 prescription drug prior authorization or. Use the tools and resources. Web to request your medical record, submit your medical records authorization form online (available in english, spanish or chinese) or sign in to my health online. Use your zip code to find your personal plan.
Sign It In A Few Clicks.
Web get the sutter health prior authorization form accomplished. Web edit your sutter health release of information online. Submit the completed and signed form by: Commercial hmo claims submission sutter health plus p.o.
Web Authorization For Use And Disclosure Of Health Information Patient Name:
Web please complete this form if you wish to authorize sutter health plus to disclose your protected health information to another individual or entity. Web rosters and referral forms. Emailing the form to mhosupport@sutterhealth.org. Ad register and subscribe now to work on sutter health radiology images release auth form.