Ssa 1763 Form
Ssa 1763 Form - Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. To the social security agency of a foreign country, to carry out the purpose of an international social security agreement entered into between the united states and the other country, pursuant to section 233 of the social security act. Fee agreement for representation before the social security administration: Use fill to complete blank online medicare & medicaid pdf forms for free. Section 1838(b) and 1818a(c)(2)(b) of the social security act require filing of notice advising the administration when termination of medicare coverage is requested. Petition for authorization to charge and collect a fee for services before the social security administration: Who can use this form? Web credit card payment form: However, you may need to have a personal interview with social security to review the risks of dropping coverage and to assist you with your request. Once completed you can sign your fillable form or send for signing.
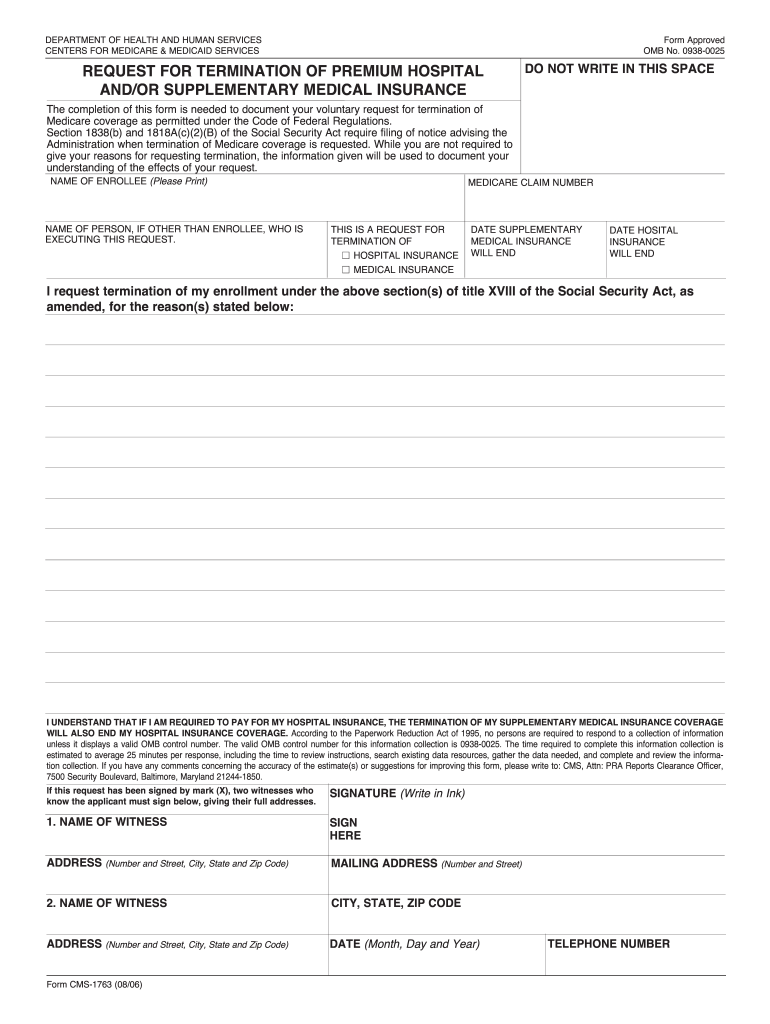
Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Once completed you can sign your fillable form or send for signing. Web the part b cancellation process begins with downloading and printing form cms 1763, but don’t fill it out yet. People with medicare premium part a or b who would like to terminate their hospital or medical. All forms are printable and downloadable. Fee agreement for representation before the social security administration: Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. The centers for medicare & medicaid services (cms) requires, when possible, a personal interview be conducted with everyone who wishes to terminate entitlement. To the department of state and its agents for administering the act in foreign countries Use fill to complete blank online medicare & medicaid pdf forms for free.
Once completed you can sign your fillable form or send for signing. You’ll need to complete the form during an interview with a representative of the social security administration (ssa) by phone or in person. To the department of state and its agents for administering the act in foreign countries All forms are printable and downloadable. However, you may need to have a personal interview with social security to review the risks of dropping coverage and to assist you with your request. Who can use this form? Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. People with medicare premium part a or b who would like to terminate their hospital or medical. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Web credit card payment form:

Medicare Part B Enrollment Form Cms L564 Form Resume Examples
The centers for medicare & medicaid services (cms) requires, when possible, a personal interview be conducted with everyone who wishes to terminate entitlement. All forms are printable and downloadable. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. People with medicare premium part a or b who would like to terminate their hospital or.
Form SSA1696 Fill Out, Sign Online and Download Fillable PDF
However, you may need to have a personal interview with social security to review the risks of dropping coverage and to assist you with your request. Fee agreement for representation before the social security administration: Who can use this form? To the department of state and its agents for administering the act in foreign countries Section 1838(b) and 1818a(c)(2)(b) of.
Social Security 1099 Form Pdf Form Resume Examples qb1VND61R2
Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Who can use this form? Petition for authorization to charge and collect a fee for services before the social security administration: To the social security agency of a foreign country, to carry out the purpose of an international social security agreement entered into between the.

Fill Free fillable Form CMS1763 REQUEST FOR TERMINATION OF PREMIUM
Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. You’ll need to complete the form during an interview with a representative of the social security administration (ssa) by phone or in person. The centers for medicare & medicaid services (cms) requires, when possible,.

Ssa 561 Printable Form Master of Documents
All forms are printable and downloadable. To the social security agency of a foreign country, to carry out the purpose of an international social security agreement entered into between the united states and the other country, pursuant to section 233 of the social security act. The centers for medicare & medicaid services (cms) requires, when possible, a personal interview be.
Medicare Part B Form Cms 1763 Form Resume Examples X42M4aXaVk
Once completed you can sign your fillable form or send for signing. Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. The centers for medicare & medicaid services (cms) requires, when possible, a personal interview be conducted with everyone who wishes to terminate.
Ssa.gov Medicare Part B Forms Form Resume Examples o7Y3kxMYBN
Web the part b cancellation process begins with downloading and printing form cms 1763, but don’t fill it out yet. Web credit card payment form: Petition for authorization to charge and collect a fee for services before the social security administration: All forms are printable and downloadable. Once completed you can sign your fillable form or send for signing.
CMS1763 2006 Fill and Sign Printable Template Online US Legal Forms
All forms are printable and downloadable. The centers for medicare & medicaid services (cms) requires, when possible, a personal interview be conducted with everyone who wishes to terminate entitlement. Who can use this form? Web the part b cancellation process begins with downloading and printing form cms 1763, but don’t fill it out yet. Web the completion of this form.

2023 SSA Gov Forms Fillable, Printable PDF & Forms Handypdf
Petition for authorization to charge and collect a fee for services before the social security administration: You can voluntarily terminate your medicare part b (medical insurance). Use fill to complete blank online medicare & medicaid pdf forms for free. Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under.
Social Security Medicare Form Cms 1763 Form Resume Examples wRYPwQW394
Once completed you can sign your fillable form or send for signing. Use fill to complete blank online medicare & medicaid pdf forms for free. To the social security agency of a foreign country, to carry out the purpose of an international social security agreement entered into between the united states and the other country, pursuant to section 233 of.
Section 1838(B) And 1818A(C)(2)(B) Of The Social Security Act Require Filing Of Notice Advising The Administration When Termination Of Medicare Coverage Is Requested.
To the department of state and its agents for administering the act in foreign countries Web credit card payment form: Fee agreement for representation before the social security administration: All forms are printable and downloadable.
You’ll Need To Complete The Form During An Interview With A Representative Of The Social Security Administration (Ssa) By Phone Or In Person.
Once completed you can sign your fillable form or send for signing. However, you may need to have a personal interview with social security to review the risks of dropping coverage and to assist you with your request. You can voluntarily terminate your medicare part b (medical insurance). Petition for authorization to charge and collect a fee for services before the social security administration:
Web The Completion Of This Form Is Needed To Document Your Voluntary Request For Termination Of Medicare Coverage As Permitted Under The Code Of Federal Regulations.
Use fill to complete blank online medicare & medicaid pdf forms for free. The centers for medicare & medicaid services (cms) requires, when possible, a personal interview be conducted with everyone who wishes to terminate entitlement. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. To the social security agency of a foreign country, to carry out the purpose of an international social security agreement entered into between the united states and the other country, pursuant to section 233 of the social security act.
People With Medicare Premium Part A Or B Who Would Like To Terminate Their Hospital Or Medical.
Who can use this form? Web the part b cancellation process begins with downloading and printing form cms 1763, but don’t fill it out yet.