Ssa 11 Bk Form
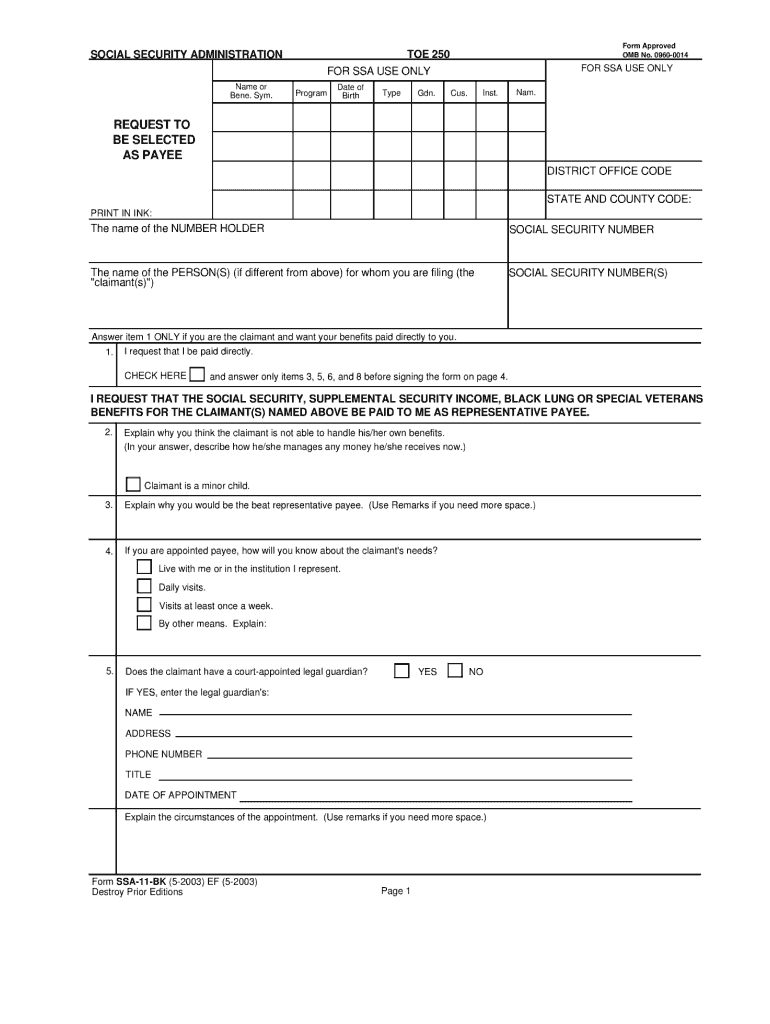
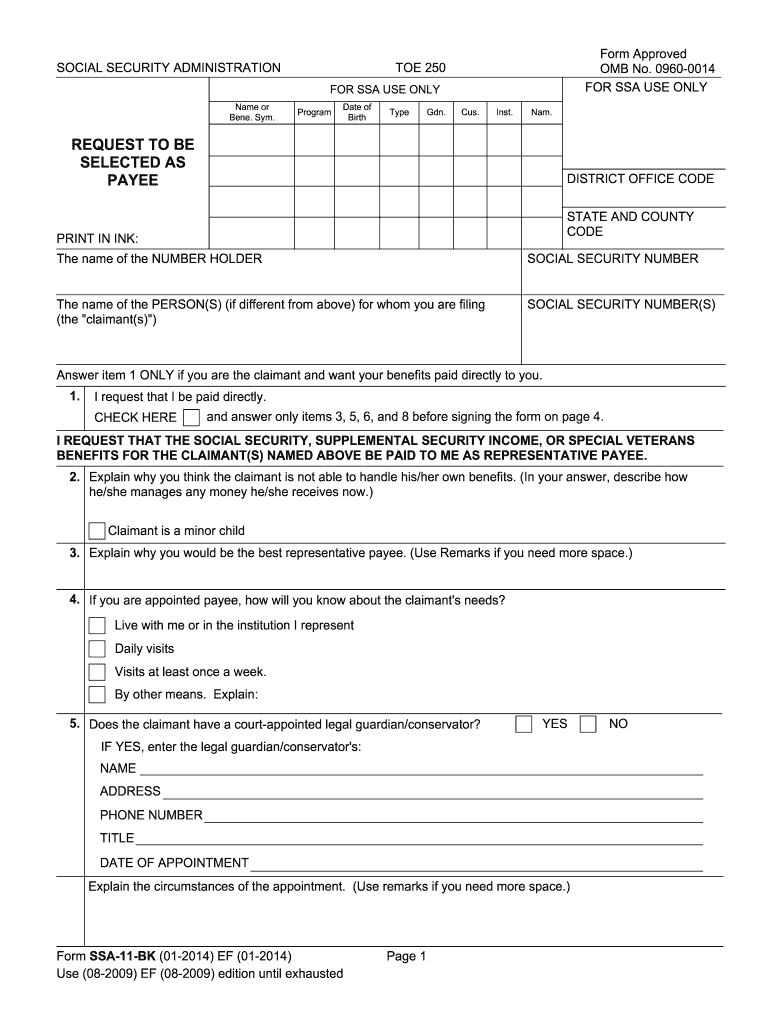
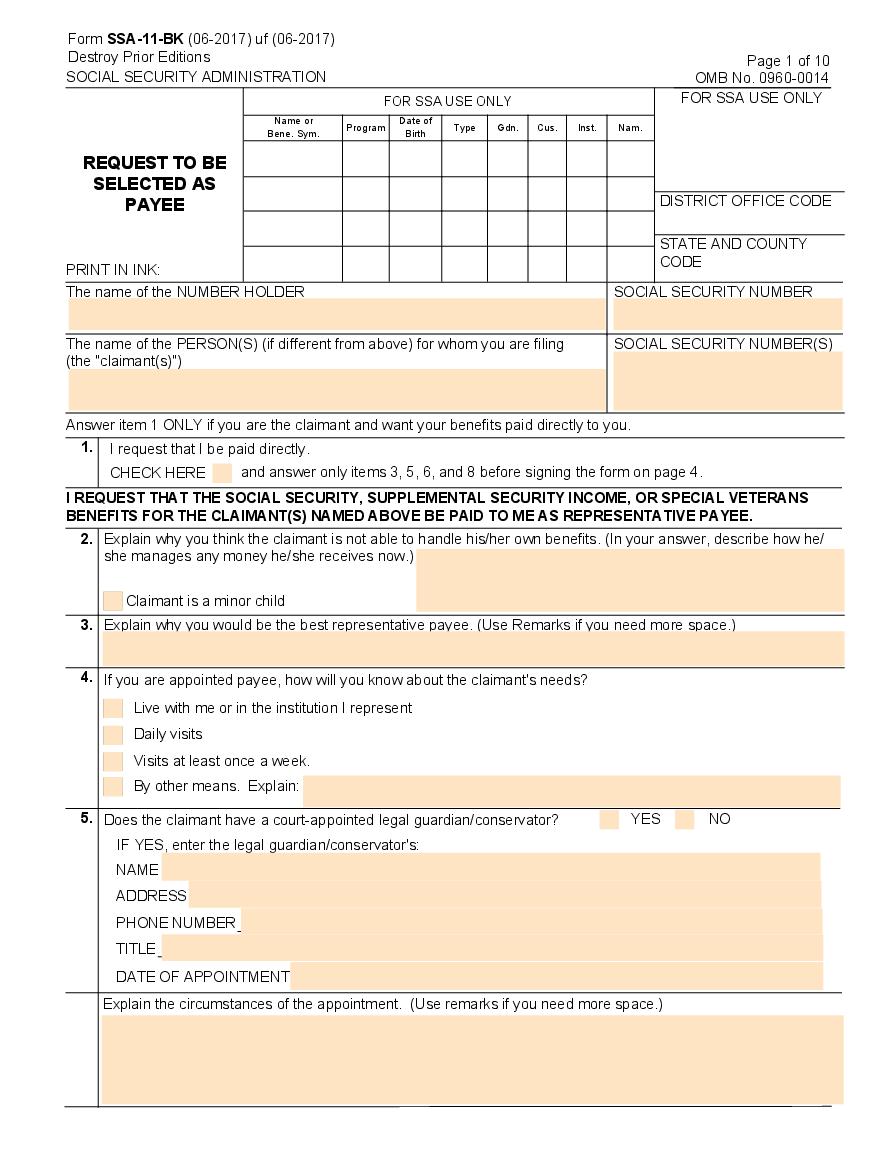
Ssa 11 Bk Form - The purpose of this form is to another person be named as payee other than the payee. Solicitud para beneficios de seguro como cónyuge: Check here and answer only items 3, 5, 6, and 8 before signing the form on page 4. Indication if you are the claimant and what your benefits paid directly to you. I request that i be paid directly. I request that the social security, supplemental security income, or special veterans benefits for the claimant(s) named above be paid to me as representative payee. I request that the social security, supplemental security income, or special veterans benefits for the claimant(s) named above be paid to me as representative payee. Signature of witness address (number and street, city, state and zip code) name of county 2. Program date of birth type gdn. Check here and answer only items 3, 5, 6, and 8 before signing the form on page 4.
Use the paper form only , when it is not possible to use erps. Application for wife's or husband's insurance benefits: Solicitud para beneficios de seguro por jubliación: Check here and answer only items 3, 5, 6, and 8 before signing the form on page 4. I request that the social security, supplemental security income, or special veterans benefits for the claimant(s) named above be paid to me as representative payee. Application for retirement insurance benefits: Name of the number holder. This form is used when the original payee is unable to manage their own finances. Program date of birth type gdn. (refer to gn 00502.113, gn 00502.115, and gn 00505.010.)
Indication if you are the claimant and what your benefits paid directly to you. Solicitud para beneficios de seguro por jubliación: I request that i be paid directly. Solicitud para beneficios de seguro como cónyuge: I request that i be paid directly. Check here and answer only items 3, 5, 6, and 8 before signing the form on page 4. (refer to gn 00502.113, gn 00502.115, and gn 00505.010.) I request that the social security, supplemental security income, or special veterans benefits for the claimant(s) named above be paid to me as representative payee. Signature of witness address (number and street, city, state and zip code) name of county 2. Name of the person (s) for whom you are filing (claimant) claimant's social security number.

Application Form Application Form Ssa11
I request that the social security, supplemental security income, or special veterans benefits for the claimant(s) named above be paid to me as representative payee. Application for retirement insurance benefits: Name of the number holder. Indication if you are the claimant and what your benefits paid directly to you. Check here and answer only items 3, 5, 6, and 8.
Ssa 11 Fill Online, Printable, Fillable, Blank pdfFiller
I request that i be paid directly. I request that the social security, supplemental security income, or special veterans benefits for the claimant(s) named above be paid to me as representative payee. Solicitud para beneficios de seguro como cónyuge: Use the paper form only , when it is not possible to use erps. Check here and answer only items 3,.
2014 Form SSA11BK Fill Online, Printable, Fillable, Blank pdfFiller
Check here and answer only items 3, 5, 6, and 8 before signing the form on page 4. I request that the social security, supplemental security income, or special veterans benefits for the claimant(s) named above be paid to me as representative payee. This form is used when the original payee is unable to manage their own finances. Check here.
Form SSA11BK Download Printable PDF or Fill Online Request to Be
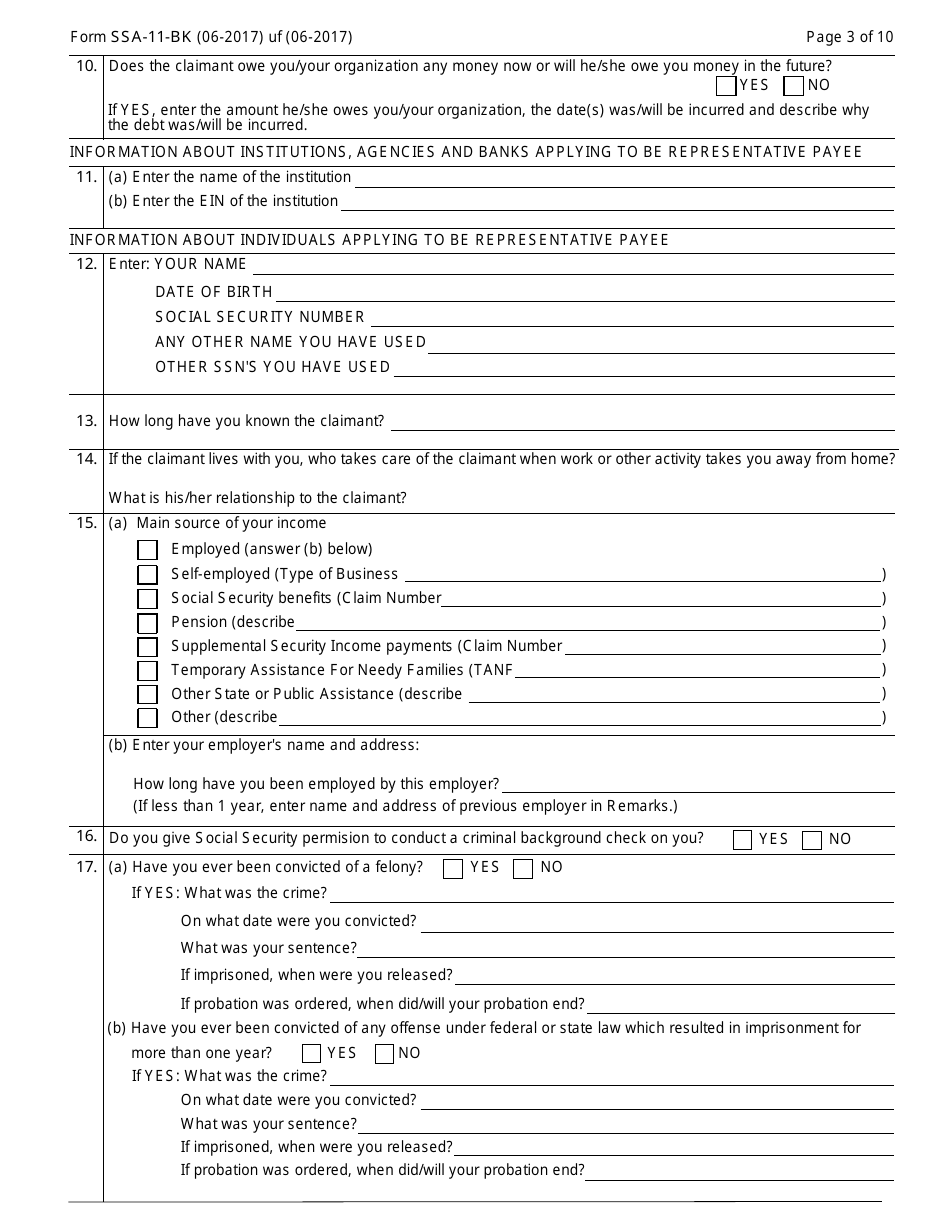
Application for wife's or husband's insurance benefits: Name of the person (s) for whom you are filing (claimant) claimant's social security number. Check here and answer only items 3, 5, 6, and 8 before signing the form on page 4. Solicitud para beneficios de seguro por jubliación: Solicitud para beneficios de seguro como cónyuge:
Ssa 11 Form Printable Optimize tax document workflows airSlate
Application for wife's or husband's insurance benefits: (refer to gn 00502.113, gn 00502.115, and gn 00505.010.) Program date of birth type gdn. I request that the social security, supplemental security income, or special veterans benefits for the claimant(s) named above be paid to me as representative payee. Name of the person (s) for whom you are filing (claimant) claimant's social.
Form SSA11BK Download Printable PDF or Fill Online Request to Be
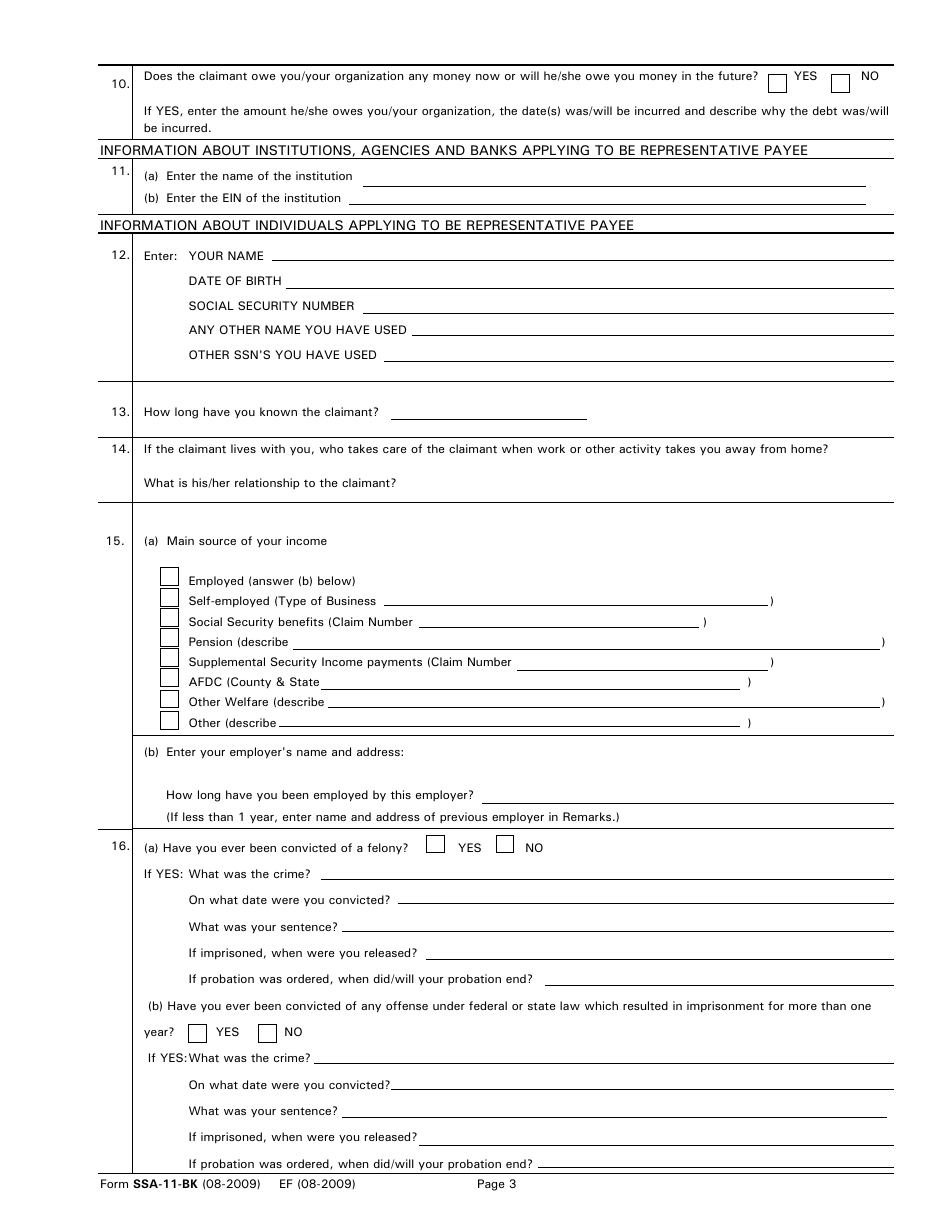
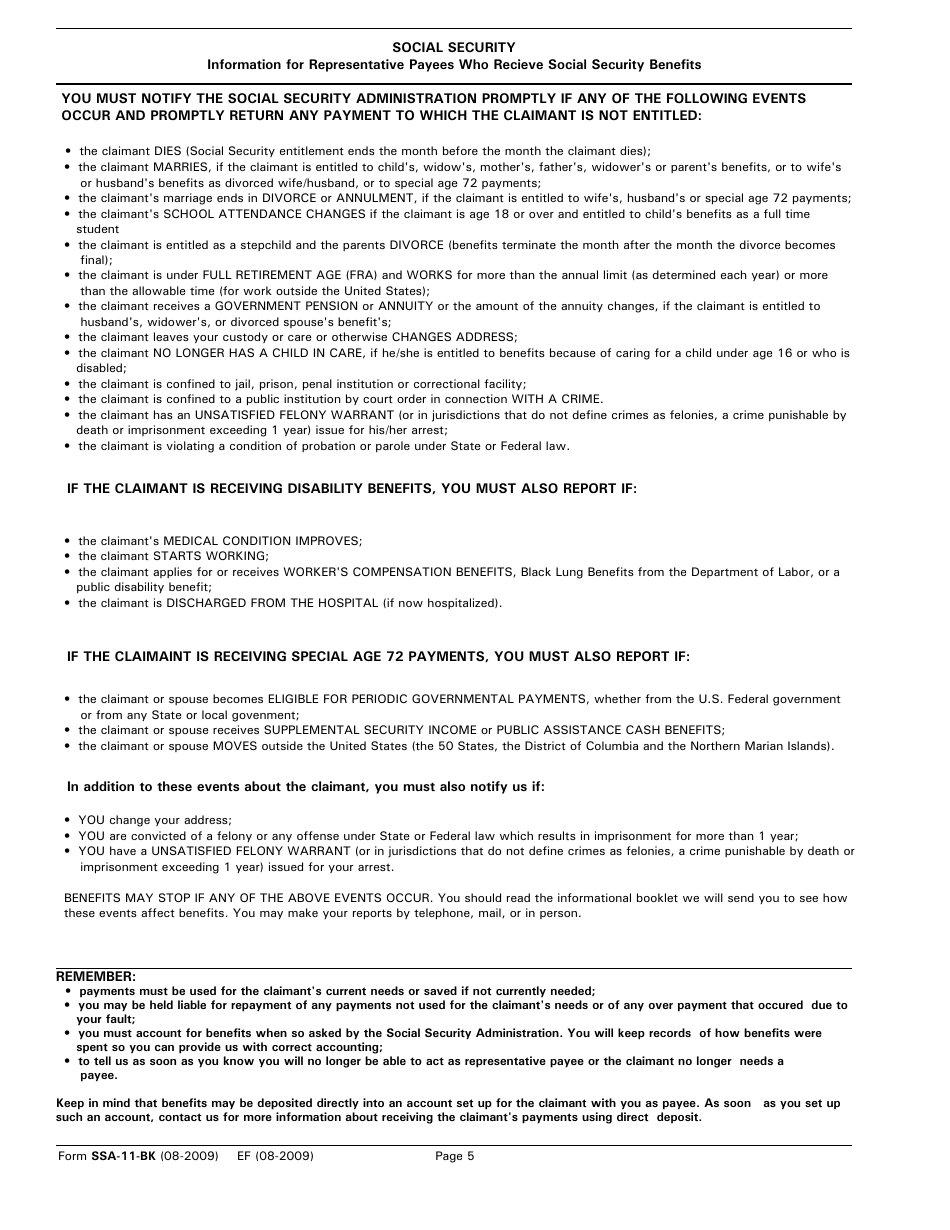
Use the paper form only , when it is not possible to use erps. Indication if you are the claimant and what your benefits paid directly to you. Signature of witness address (number and street, city, state and zip code) social security information for representative payees who receive social security benefits. Signature of witness address (number and street, city, state.
Form SSA1BK Edit, Fill, Sign Online Handypdf
The purpose of this form is to another person be named as payee other than the payee. Signature of witness address (number and street, city, state and zip code) name of county 2. For example, we must take paper applications for applicants who do not have a social security number (ssn). Solicitud para beneficios de seguro por jubliación: This form.

Printable Ssa 11 Bk Master of Documents
Signature of witness address (number and street, city, state and zip code) name of county 2. I request that i be paid directly. I request that i be paid directly. Application for wife's or husband's insurance benefits: (refer to gn 00502.113, gn 00502.115, and gn 00505.010.)
Form SSA11BK Download Fillable PDF or Fill Online Request to Be
Program date of birth type gdn. Solicitud para beneficios de seguro como cónyuge: Signature of witness address (number and street, city, state and zip code) social security information for representative payees who receive social security benefits. I request that i be paid directly. I request that the social security, supplemental security income, or special veterans benefits for the claimant(s) named.

Free fillable Form SSA11BK REQUEST TO BE SELECTED AS PAYEE (SOCIAL
The purpose of this form is to another person be named as payee other than the payee. Name of the number holder. Application for retirement insurance benefits: Indication if you are the claimant and what your benefits paid directly to you. Solicitud para beneficios de seguro como cónyuge:
This Form Is Used When The Original Payee Is Unable To Manage Their Own Finances.
Name of the person (s) for whom you are filing (claimant) claimant's social security number. Use the paper form only , when it is not possible to use erps. Check here and answer only items 3, 5, 6, and 8 before signing the form on page 4. I request that the social security, supplemental security income, or special veterans benefits for the claimant(s) named above be paid to me as representative payee.
I Request That I Be Paid Directly.
For example, we must take paper applications for applicants who do not have a social security number (ssn). Application for retirement insurance benefits: The purpose of this form is to another person be named as payee other than the payee. Name of the number holder.
Solicitud Para Beneficios De Seguro Como Cónyuge:
Application for wife's or husband's insurance benefits: Signature of witness address (number and street, city, state and zip code) name of county 2. I request that i be paid directly. Indication if you are the claimant and what your benefits paid directly to you.
Program Date Of Birth Type Gdn.
(refer to gn 00502.113, gn 00502.115, and gn 00505.010.) Signature of witness address (number and street, city, state and zip code) social security information for representative payees who receive social security benefits. Check here and answer only items 3, 5, 6, and 8 before signing the form on page 4. Solicitud para beneficios de seguro por jubliación: