Prescription Order Form
Prescription Order Form - Prior to submission, the following items (indicated with a **) must be completed. Web new home delivery prescription order form 1. Web this order form is required every time a written prescription from your medical provider is mailed. Do not send cash in the mail. Just check the medications you want to refill and mail the form back to our mail order pharmacy, along with a check or your credit card information. Patient medicaid number (if available) patient full name To manage your prescriptions, sign inor register. Web mail order prescription physician fax form. Web this prescription request form template contains form fields that ask for the patient's name, age, date of birth, and contact details. Member id number (additional coverage, if applicable) secondary member id number last name first name mi delivery address apt.
Web monday, october 4, 2021 dhcf prescription order form (pof) district of columbia dhcf prescription order form (pof)for long term care services and supports attachment (s): Web this order form is required every time a written prescription from your medical provider is mailed. Our pharmacists are available 24/7 from the privacy of your home. Member and physician information — please use black or blue ink. Medication delivery may take up to 21 days from the date you mail your order. This form is to be completed by the patient, family member, or caregiver with power of attorney. Use a separate form for each patient or family member. Print plan formsdownload a form to start a new mail order prescription. Once we have your prescription, we’ll take care of the rest. Easy refillrefill prescriptions (mail service only) without creating an account.
# city state zip code phone number with area code Medication delivery may take up to 21 days from the date you mail your order. Use a separate form for each patient or family member. Our pharmacists are available 24/7 from the privacy of your home. Print plan formsdownload a form to start a new mail order prescription. Patient medicaid number (if available) patient full name Do not send cash in the mail. Verify the medication is covered by your patient’s health care plan or if it will require a prior authorization Web how it works transfer your prescription log in or register to get started. Just check the medications you want to refill and mail the form back to our mail order pharmacy, along with a check or your credit card information.
Blank Prescription Form Template
Once we have your prescription, we’ll take care of the rest. Web mail order prescription physician fax form. Do not send cash in the mail. Web how it works transfer your prescription log in or register to get started. Talk to a pharmacist have questions?
44+ Blank Order Form Templates PDF, DOC, Excel Free & Premium Templates
Member id number (additional coverage, if applicable) secondary member id number last name first name mi delivery address apt. Print plan formsdownload a form to start a new mail order prescription. Do not send cash in the mail. Our pharmacists are available 24/7 from the privacy of your home. # city state zip code phone number with area code

PRESCRIPTION FORMS 20101 123print.ca
Before you send us a prescription and to minimize any delays or outreach… verify with your patient optumrx is their home delivery pharmacy; Web how it works transfer your prescription log in or register to get started. Verify the medication is covered by your patient’s health care plan or if it will require a prior authorization Do not send cash.
2010 prescription order form
To manage your prescriptions, sign inor register. Web this order form is required every time a written prescription from your medical provider is mailed. Verify the medication is covered by your patient’s health care plan or if it will require a prior authorization Use a separate form for each patient or family member. This form is to be completed by.
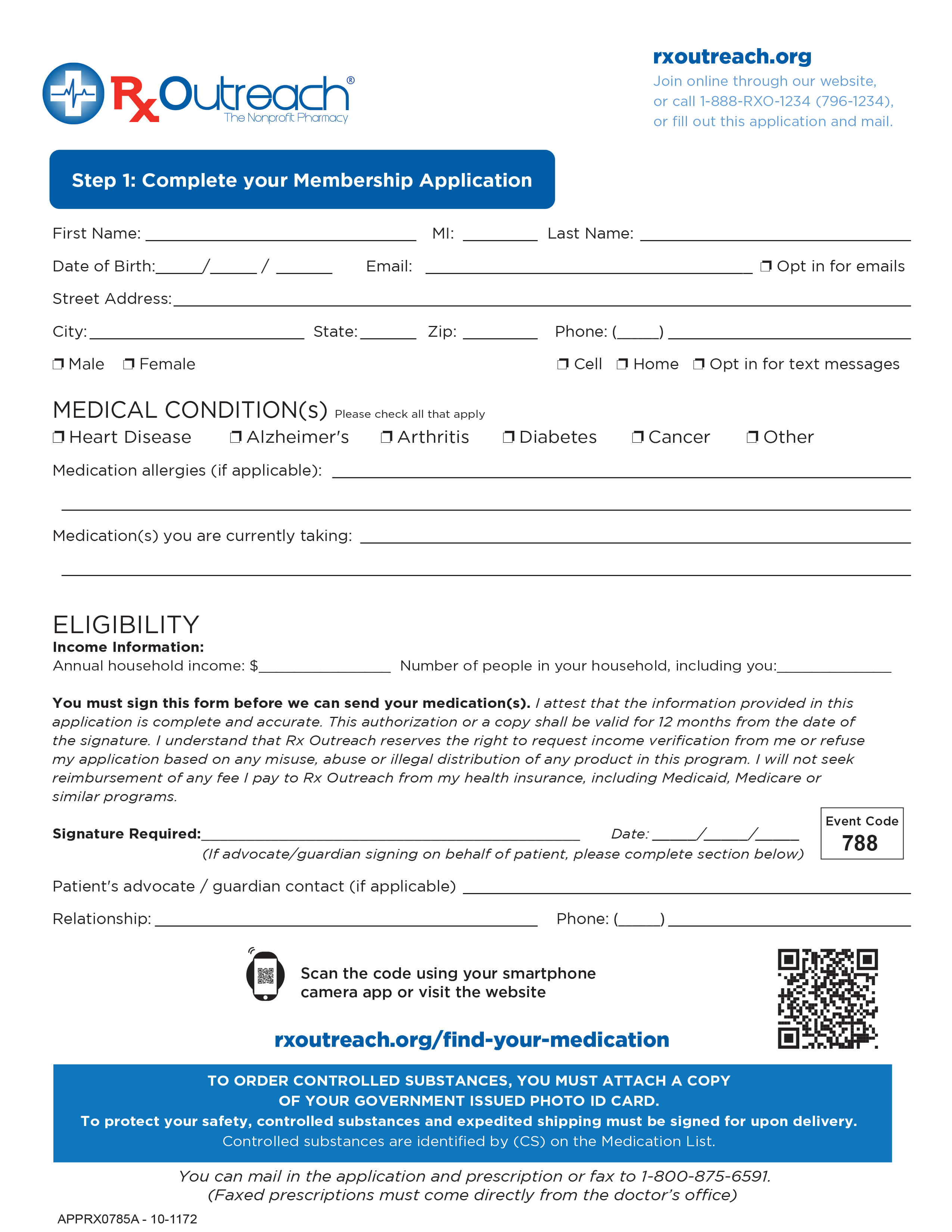
Patient Forms Rx Outreach
Patient medicaid number (if available) patient full name Web mail order prescription physician fax form. Print plan formsdownload a form to start a new mail order prescription. # city state zip code phone number with area code Member and physician information — please use black or blue ink.
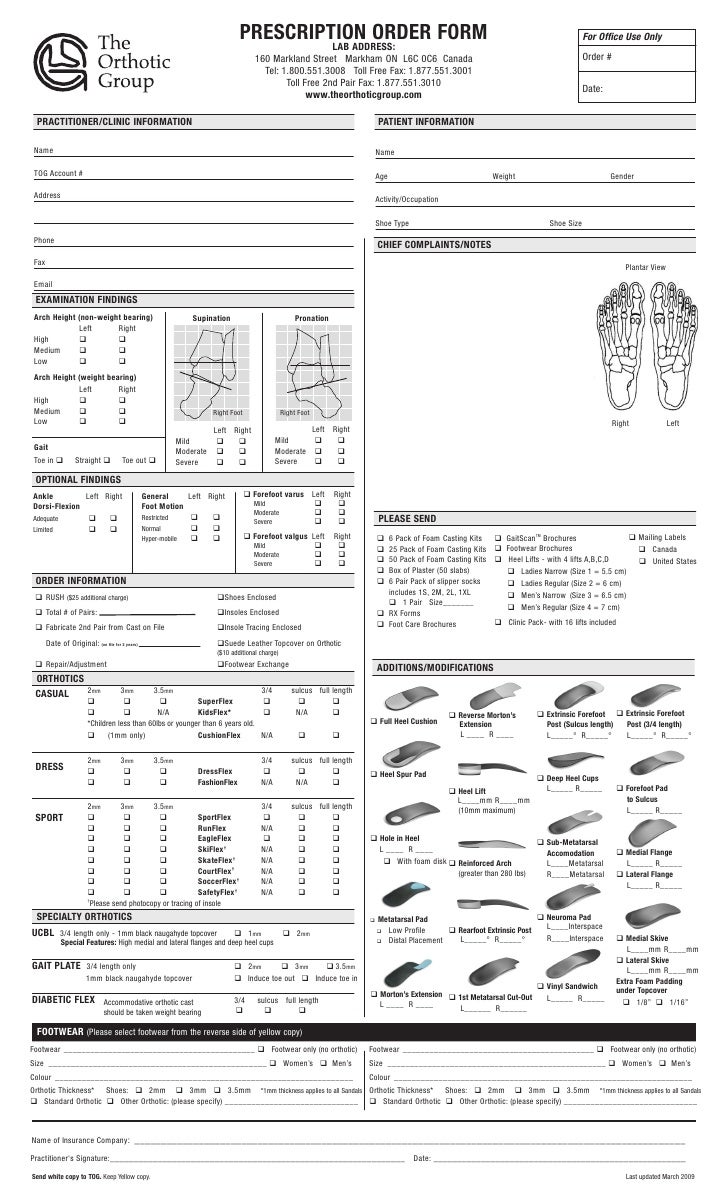
14+ Prescription Templates Templates Front
Talk to a pharmacist have questions? This template also verifies the physician's name, prescribed medications, pharmacy name, special instructions, confirmation, and signature. This form is to be completed by the patient, family member, or caregiver with power of attorney. Our pharmacists are available 24/7 from the privacy of your home. Web this prescription request form template contains form fields that.
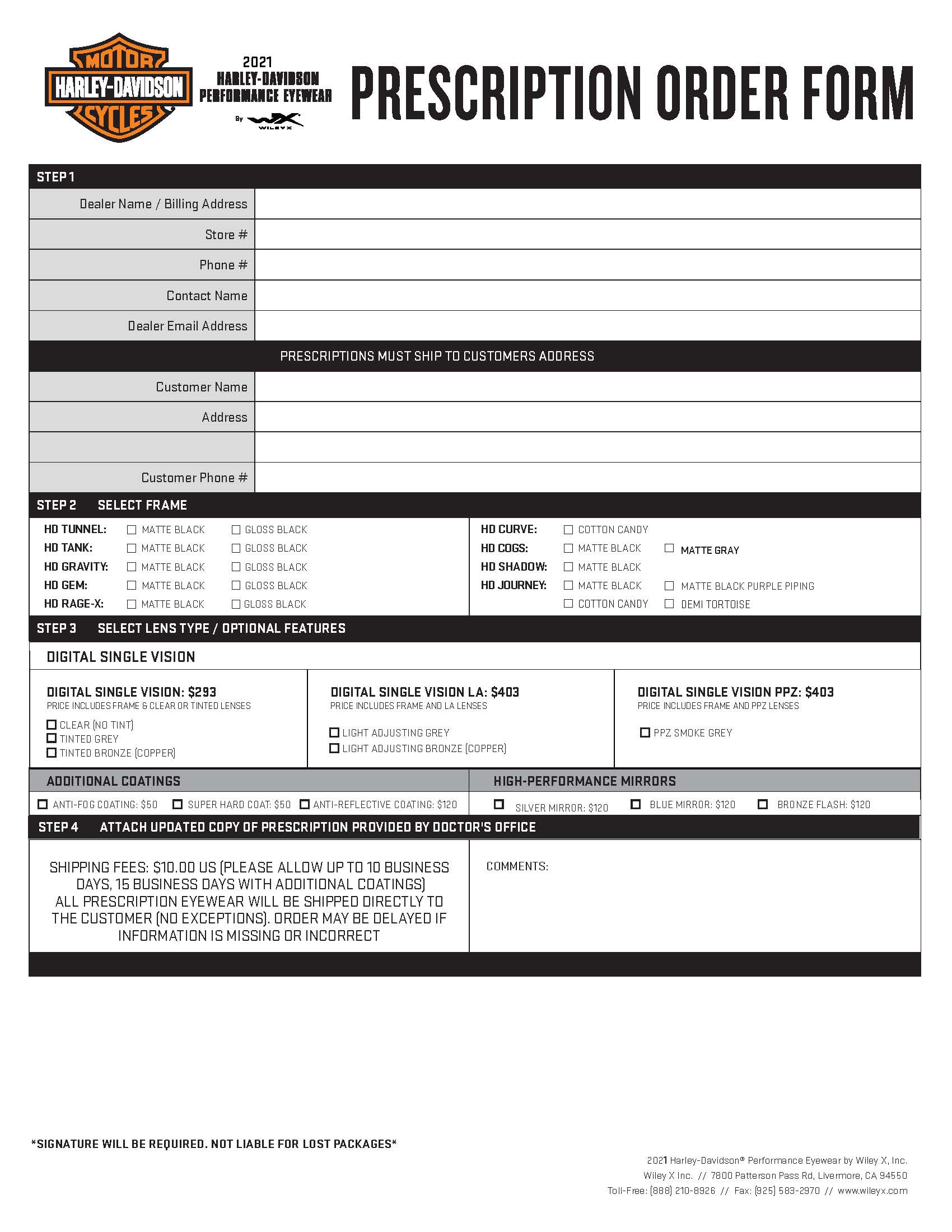
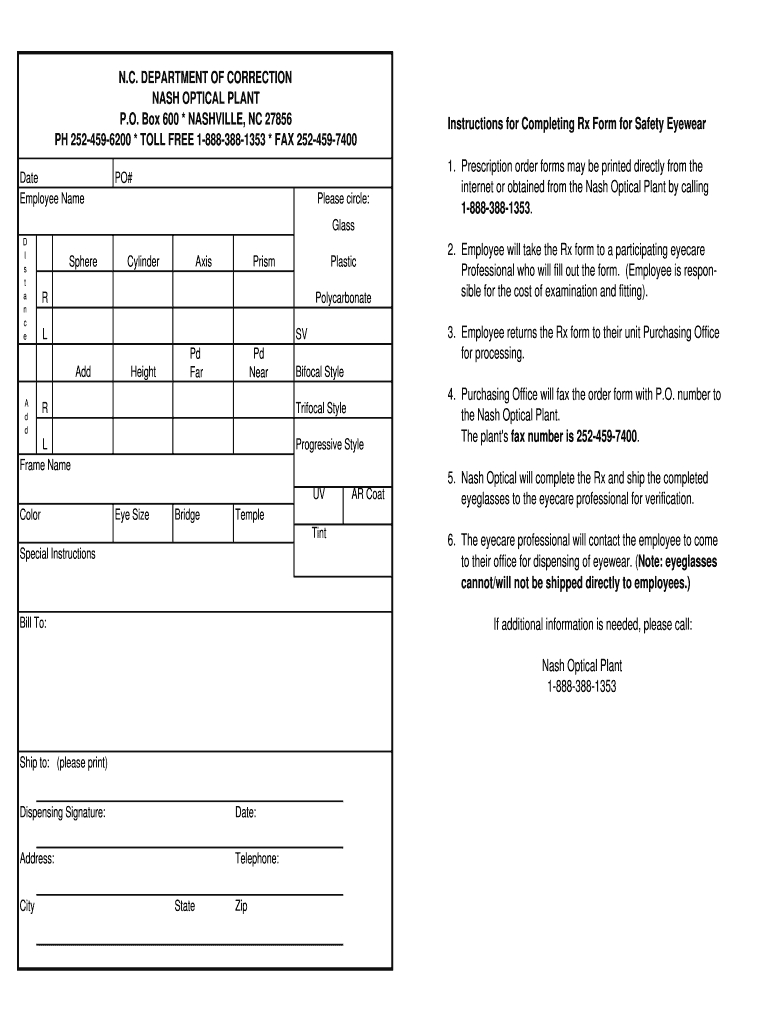
HD Eyewear
Patient medicaid number (if available) patient full name Use a separate form for each patient or family member. Web this prescription request form template contains form fields that ask for the patient's name, age, date of birth, and contact details. Web mail order prescription physician fax form. Web monday, october 4, 2021 dhcf prescription order form (pof) district of columbia.
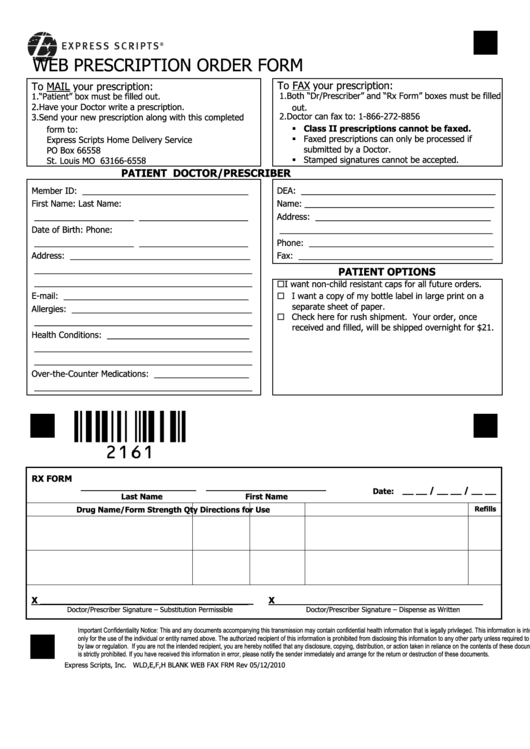
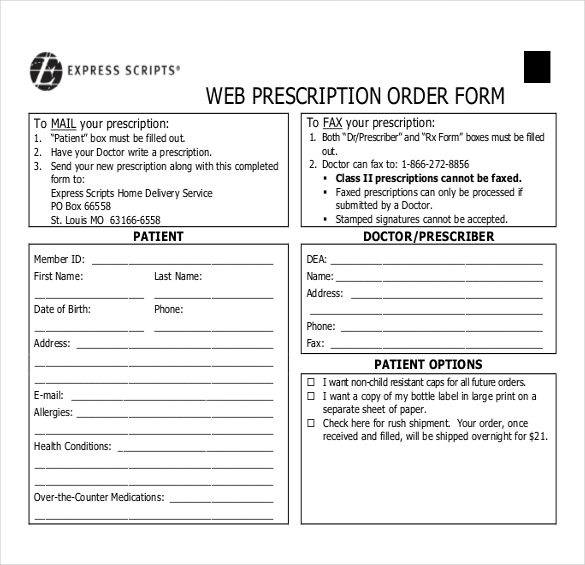
Top 16 Express Scripts Forms And Templates free to download in PDF format
Web this prescription request form template contains form fields that ask for the patient's name, age, date of birth, and contact details. Easy refillrefill prescriptions (mail service only) without creating an account. Before you send us a prescription and to minimize any delays or outreach… verify with your patient optumrx is their home delivery pharmacy; Web monday, october 4, 2021.

Glasses Prescription Order Form Infab
Prior to submission, the following items (indicated with a **) must be completed. Our pharmacists are available 24/7 from the privacy of your home. Just check the medications you want to refill and mail the form back to our mail order pharmacy, along with a check or your credit card information. Verify the medication is covered by your patient’s health.
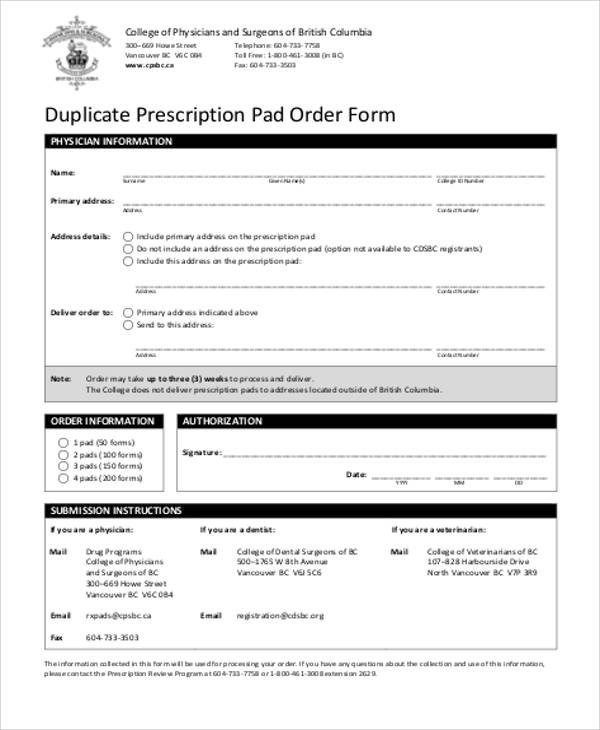
FREE 6+ Sample Duplicate Order Forms in MS Word PDF
Web new home delivery prescription order form 1. This form is to be completed by the patient, family member, or caregiver with power of attorney. Web mail order prescription physician fax form. Our pharmacists are available 24/7 from the privacy of your home. This template also verifies the physician's name, prescribed medications, pharmacy name, special instructions, confirmation, and signature.
This Template Also Verifies The Physician's Name, Prescribed Medications, Pharmacy Name, Special Instructions, Confirmation, And Signature.
Do not send cash in the mail. Our pharmacists are available 24/7 from the privacy of your home. Print plan formsdownload a form to start a new mail order prescription. Web this prescription request form template contains form fields that ask for the patient's name, age, date of birth, and contact details.
Easy Refillrefill Prescriptions (Mail Service Only) Without Creating An Account.
Web new home delivery prescription order form 1. Member id number (additional coverage, if applicable) secondary member id number last name first name mi delivery address apt. This form is to be completed by the patient, family member, or caregiver with power of attorney. Web this order form is required every time a written prescription from your medical provider is mailed.
Web Monday, October 4, 2021 Dhcf Prescription Order Form (Pof) District Of Columbia Dhcf Prescription Order Form (Pof)For Long Term Care Services And Supports Attachment (S):
Talk to a pharmacist have questions? To manage your prescriptions, sign inor register. # city state zip code phone number with area code Just check the medications you want to refill and mail the form back to our mail order pharmacy, along with a check or your credit card information.
Medication Delivery May Take Up To 21 Days From The Date You Mail Your Order.
Use a separate form for each patient or family member. Once we have your prescription, we’ll take care of the rest. Verify the medication is covered by your patient’s health care plan or if it will require a prior authorization Prior to submission, the following items (indicated with a **) must be completed.