Molina Appeals Form
Molina Appeals Form - Web to file your appeal, you can: Web if molina medicare or one of our plan providers refuses to give you a service you think should be covered, you can file an appeal. Molina healthcare grievance and appeals unit p.o. Appeal request form for services being reduced, suspended, or stopped mail to: Web provider claims appeal request form provider information: Web by submitting my information via this form, i consent to having molina healthcare collect my personal information. Stop, suspend, reduce or deny a service or; If molina medicare or one of our plan. Web an appeal can be filed when you do not agree with molina medicare’s decision to: Stop, suspend, reduce or deny a service or;
Molina healthcare of new york, inc. Web you may contact a molina complaints and appeals coordinator at the number listed on the acknowledgement letter or notice of adverse benefit determination or final adverse. Web to file your appeal, you can: / / • please submit the request by our preferred method, visiting the provider portal, by visiting. Web claim reconsideration request form date: Web member grievance and appeal procedure molina healthcare’s grievance and appeal procedure is overseen by our grievance and appeal unit.its purpose is to resolve. Web by submitting my information via this form, i consent to having molina healthcare collect my personal information. Deny payment for services provided. Web an appeal can be filed when you do not agree with molina medicare’s decision to: Molina healthcare grievance and appeals unit p.o.
Deny payment for services provided. Web an appeal can be filed when you do not agree with molina medicare’s decision to: Appeals & grievances department or by mail to. Web provider claims appeal request form provider information: Box 4004 bothell, wa 98041 molinamarketplace.com we will send you a letter acknowledging receipt of your. Web an appeal can be filed when you do not agree with molina medicare’s decision to: If molina medicare or one of our plan. Molina healthcare of new york, inc. Web by submitting my information via this form, i consent to having molina healthcare collect my personal information. Web provider appeals the molina healthcare of michigan appeals team coordinates clinical review for provider appeals with molina healthcare medical.
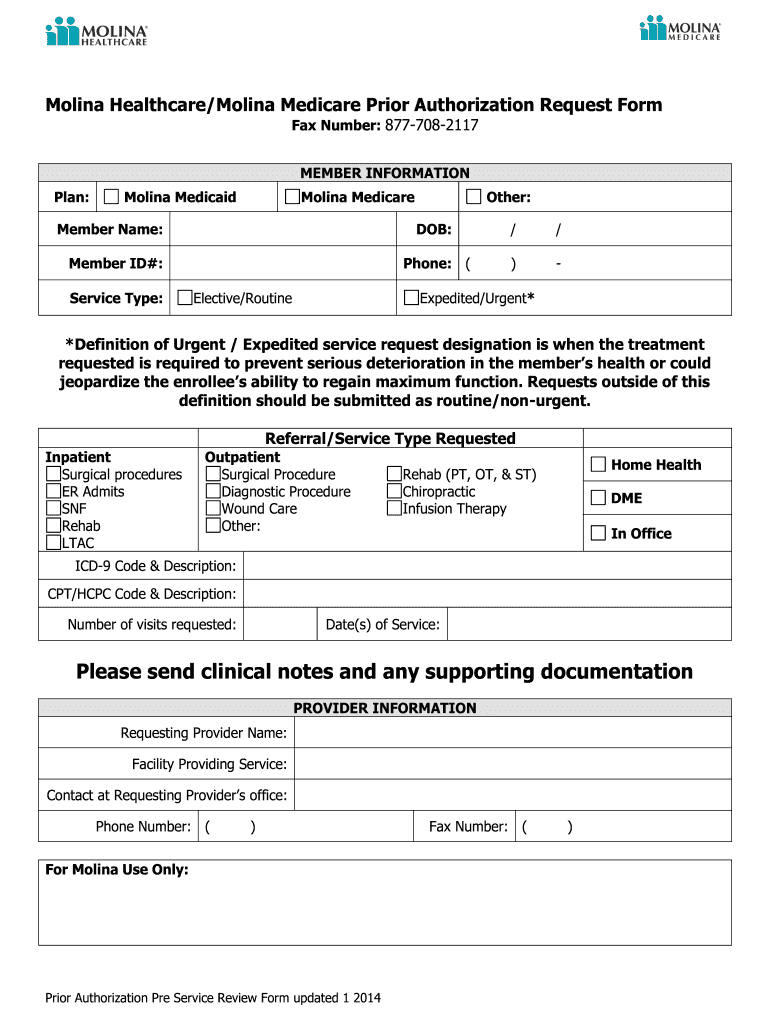
Molina Healthcare Medicare Prior Authorization Request 2014 Fill and
Web provider appeals the molina healthcare of michigan appeals team coordinates clinical review for provider appeals with molina healthcare medical. Deny payment for services provided. If molina medicare or one of our plan. Web by submitting my information via this form, i consent to having molina healthcare collect my personal information. Stop, suspend, reduce or deny a service or;
Fax Fill Out and Sign Printable PDF Template signNow
Web an appeal can be filed when you do not agree with molina medicare’s decision to: Stop, suspend, reduce or deny a service or; Deny payment for services provided. Stop, suspend, reduce or deny a service or; Web if molina medicare or one of our plan providers refuses to give you a service you think should be covered, you can.
MOLINA HEALTHCARE, INC. FORM 8K EX99.2 January 26, 2011
Web to file your appeal, you can: Web claim reconsideration request form date: Web provider claims appeal request form provider information: Deny payment for services provided. Web an appeal can be filed when you do not agree with molina medicare’s decision to:

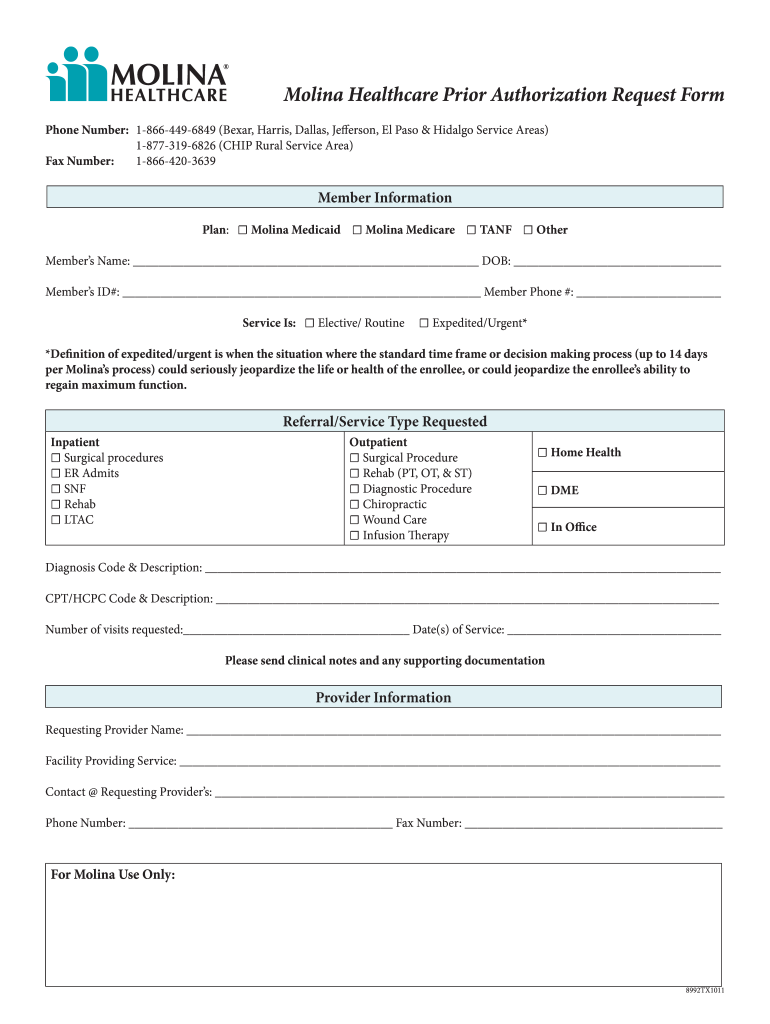
Molina Medicare Pa Forms Universal Network
Appeals & grievances department or by mail to. 711) write a letter to: Web as a molina healthcare member, if you have a problem with your medical care or our services, you have a right to file a complaint (grievance) or appeal. Web you may contact a molina complaints and appeals coordinator at the number listed on the acknowledgement letter.
Molina Prior Authorization Form 2021 Fill Online, Printable, Fillable
Appeal request form for services being reduced, suspended, or stopped mail to: / / • please submit the request by our preferred method, visiting the provider portal, by visiting. Molina healthcare grievance and appeals unit p.o. Molina healthcare of new york, inc. Web molina healthcare of new york, inc.

Fillable Virginia Medicaid/famis Appeal Request Form printable pdf download
Stop, suspend, reduce or deny a service or; 711) write a letter to: Box 4004 bothell, wa 98041 molinamarketplace.com we will send you a letter acknowledging receipt of your. Web member grievance and appeal procedure molina healthcare’s grievance and appeal procedure is overseen by our grievance and appeal unit.its purpose is to resolve. If molina medicare or one of our.

UT Molina Healthcare Prior Authorization Form 20162022 Fill and Sign
Molina healthcare of new york, inc. Stop, suspend, reduce or deny a service or; Web you may contact a molina complaints and appeals coordinator at the number listed on the acknowledgement letter or notice of adverse benefit determination or final adverse. Box 4004 bothell, wa 98041 molinamarketplace.com we will send you a letter acknowledging receipt of your. Web an appeal.

MOLINA HEALTHCARE, INC. FORM 8K EX99.1 January 12, 2010
Web claim reconsideration request form date: Stop, suspend, reduce or deny a service or; Web molina healthcare of new york, inc. / / • please submit the request by our preferred method, visiting the provider portal, by visiting. If molina medicare or one of our plan.

Washington Molina Marketplace Appeal Request Form. Washington Molina
Molina healthcare grievance and appeals unit p.o. Web by submitting my information via this form, i consent to having molina healthcare collect my personal information. Web if molina medicare or one of our plan providers refuses to give you a service you think should be covered, you can file an appeal. Web claim reconsideration request form date: 711) write a.

MOLINA HEALTHCARE, INC. FORM 8K EX99.1 September 16, 2011
Web submit the completed form through one of the following: / / • please submit the request by our preferred method, visiting the provider portal, by visiting. Web an appeal can be filed when you do not agree with molina medicare’s decision to: Web member grievance and appeal procedure molina healthcare’s grievance and appeal procedure is overseen by our grievance.
Web Provider Claims Appeal Request Form Provider Information:
Web an appeal can be filed when you do not agree with molina medicare’s decision to: Deny payment for services provided. Web submit the completed form through one of the following: Web to file your appeal, you can:
Web Wisconsin Provider Appeal Form Line Of Business:
Web if molina medicare or one of our plan providers refuses to give you a service you think should be covered, you can file an appeal. Web by submitting my information via this form, i consent to having molina healthcare collect my personal information. Web claim reconsideration request form date: Web provider appeals the molina healthcare of michigan appeals team coordinates clinical review for provider appeals with molina healthcare medical.
Web As A Molina Healthcare Member, If You Have A Problem With Your Medical Care Or Our Services, You Have A Right To File A Complaint (Grievance) Or Appeal.
Web you may contact a molina complaints and appeals coordinator at the number listed on the acknowledgement letter or notice of adverse benefit determination or final adverse. If molina medicare or one of our plan. 711) write a letter to: Stop, suspend, reduce or deny a service or;
/ / • Please Submit The Request By Our Preferred Method, Visiting The Provider Portal, By Visiting.
Molina healthcare of new york, inc. Appeals & grievances department or by mail to. Web an appeal can be filed when you do not agree with molina medicare’s decision to: Molina healthcare grievance and appeals unit p.o.