Medical Intake Form Pdf
Medical Intake Form Pdf - Add your logo, change the background image, or replace form. Relationship health and medical information. Web new patient medical intake form this form helps us learn about your medical history. 141.8 kb download the patient fills the intake form as this is a part of the formality of any health care center or the hospital. When did your symptoms or illness begin? Ad access millions of ebooks, audiobooks, podcasts, and more. Patient intake forms are designed to expedite the paperwork process for new and existing patients at medical practices. Web collect medical history and other information about your patients through a secure online medical intake form. With scribd, you can take your ebooks and audibooks anywhere, even offline. Web new patient intake form medical history *check all that apply+ condition you father mother sibling other w/ relation anxiety cc c c c asthma cc c c c arthritis cc c c c.
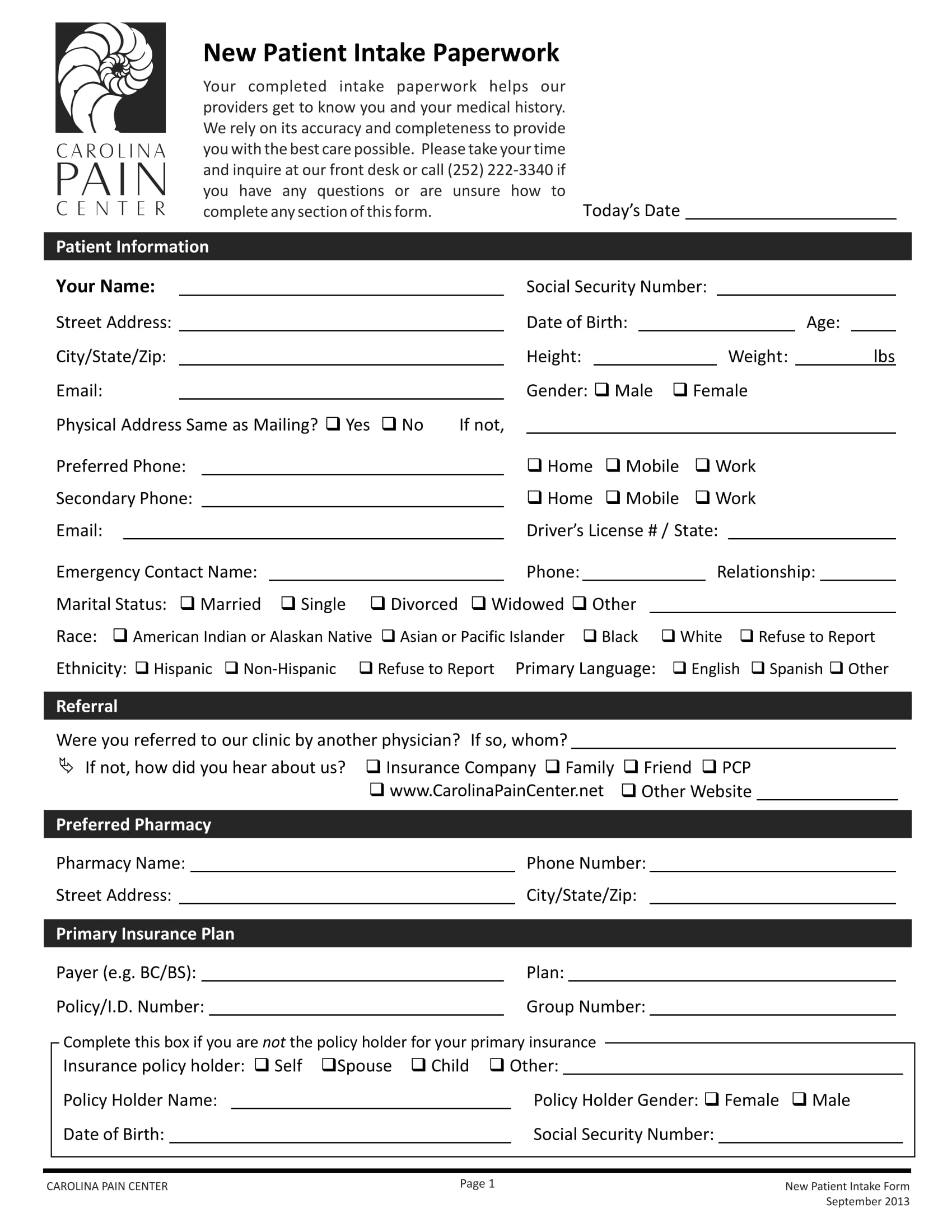
Web collect medical history and other information about your patients through a secure online medical intake form. Web free patient intake form template. List any medications and vitamins/minerals/herbs that you are currently taking. Relationship health and medical information. Ad access millions of ebooks, audiobooks, podcasts, and more. Edit, sign and save balance patient intake form. Add your logo, change the background image, or replace form. Web a medical patient intake form is used by medical professionals to collect new patients’ medical history, contact details, insurance information, and more. Web start now what is a medical intake form? Web medical intake form please complete all of the following as accurately as possible:
Web free patient intake form template. With scribd, you can take your ebooks and audibooks anywhere, even offline. 08/20 page 3 of 3 client name: When did your symptoms or illness begin? Medical intake forms collect demographic, health history, consent forms, insurance, and other important pieces of information from. Not every question is relevant to everyone. Web new patient intake form medical history *check all that apply+ condition you father mother sibling other w/ relation anxiety cc c c c asthma cc c c c arthritis cc c c c. Web medical intake form patient information patient identifier (if known) marital status zip code last name preferred pronouns. Name __________________________________ age _____ birthdate _________ sex ______. Web a medical intake form is a document used to collect information about a patient's health history, including current health problems and medications.
FREE 14+ Client Intake Forms in PDF MS Word Excel
Ad your practice, your way! Web medical intake form patient information patient identifier (if known) marital status zip code last name preferred pronouns. 08/20 page 3 of 3 client name: Expedite your intake forms process, assessments & other documentation with simplepractice. Web a medical patient intake form is used by medical professionals to collect new patients’ medical history, contact details,.
FREE 7+ Medical Intake Forms in PDF
Ad estate planning, estate planning, power of attorney, affidavits & more! Intuitive intake forms, scheduling, billing, telehealth & more. Edit, sign and save balance patient intake form. 141.8 kb download the patient fills the intake form as this is a part of the formality of any health care center or the hospital. There are forms for patient charts,.

Intake Form PDF PDF Medicine Clinical Medicine
After completing the formality only the. List any medications and vitamins/minerals/herbs that you are currently taking. Edit pdfs, create forms, collect data, collaborate with your team, secure docs and more. Web collect medical history and other information about your patients through a secure online medical intake form. Ad your practice, your way!
FREE 6+ New Patient Intake Forms in PDF MS Word Excel
Web a medical patient intake form is used by medical professionals to collect new patients’ medical history, contact details, insurance information, and more. Patient intake forms are designed to expedite the paperwork process for new and existing patients at medical practices. Web medical intake form patient information patient identifier (if known) marital status zip code last name preferred pronouns. With.
FREE 7+ Medical Intake Forms in PDF
Expedite your intake forms process, assessments & other documentation with simplepractice. Convert and save your simple medical intake form as pdf (.pdf), presentation (.pptx), image (.jpeg), spreadsheet (.xlsx) or document (.docx). Medical intake forms collect demographic, health history, consent forms, insurance, and other important pieces of information from. Edit pdfs, create forms, collect data, collaborate with your team, secure docs.
Medical intake form in Word and Pdf formats
Intuitive intake forms, scheduling, billing, telehealth & more. Add your logo, change the background image, or replace form. Web free patient intake form template. Name __________________________________ age _____ birthdate _________ sex ______. 08/20 page 3 of 3 client name:
FREE 7+ Medical Intake Forms in PDF
Web new patient intake form medical history *check all that apply+ condition you father mother sibling other w/ relation anxiety cc c c c asthma cc c c c arthritis cc c c c. Name __________________________________ age _____ birthdate _________ sex ______. Ad your practice, your way! Referred by patient information describe the reason for your visit. Convert and save.
FREE 7+ Medical Intake Forms in PDF
Edit, sign and save balance patient intake form. Web new patient intake form medical history *check all that apply+ condition you father mother sibling other w/ relation anxiety cc c c c asthma cc c c c arthritis cc c c c. Ad your practice, your way! Expedite your intake forms process, assessments & other documentation with simplepractice. Convert and.
New Patient Intake Form (Editable).pdf DocDroid
There are forms for patient charts,. 08/20 page 3 of 3 client name: Web free patient intake form template. Web medical intake form patient information patient identifier (if known) marital status zip code last name preferred pronouns. Intuitive intake forms, scheduling, billing, telehealth & more.
FREE 6+ New Patient Intake Forms in PDF MS Word Excel
There are forms for patient charts,. Web a medical intake form is a document used to collect information about a patient's health history, including current health problems and medications. Intuitive intake forms, scheduling, billing, telehealth & more. Intuitive intake forms, scheduling, billing, telehealth & more. Web start now what is a medical intake form?
Web A Medical Patient Intake Form Is Used By Medical Professionals To Collect New Patients’ Medical History, Contact Details, Insurance Information, And More.
Web medical intake form please complete all of the following as accurately as possible: These forms have been developed from a variety of sources, including acp members, for use in your practice. Web a medical intake form is a document used to collect information about a patient's health history, including current health problems and medications. Expedite your intake forms process, assessments & other documentation with simplepractice.
Web Start Now What Is A Medical Intake Form?
Ad your practice, your way! Web collect medical history and other information about your patients through a secure online medical intake form. Edit pdfs, create forms, collect data, collaborate with your team, secure docs and more. 08/20 page 3 of 3 client name:
Ad Your Practice, Your Way!
Intuitive intake forms, scheduling, billing, telehealth & more. Web free patient intake form template. Web medical intake form patient information patient identifier (if known) marital status zip code last name preferred pronouns. Expedite your intake forms process, assessments & other documentation with simplepractice.
Web New Patient Intake Form Medical History *Check All That Apply+ Condition You Father Mother Sibling Other W/ Relation Anxiety Cc C C C Asthma Cc C C C Arthritis Cc C C C.
Name __________________________________ age _____ birthdate _________ sex ______. Add your logo, change the background image, or replace form. Please complete it to the best of your ability. Ad access millions of ebooks, audiobooks, podcasts, and more.