Doh Form 4359
Doh Form 4359 - Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. The name, license number, and the complete business address must be indicated. Get your online template and fill it in using progressive features. Follow the simple instructions below: Expanded syringe access program (esap) forms; Share your form with others send doh 4359 via email, link, or fax. Patient identifying information (use additional paper if necessary) 2. If the patient was examined bya physican’s assistant, specialist’s assistant, or nurse practioner, complete the required information(pg 1). Americans with disabilities act complaint form (pdf) asbestos. Patient identifying information (use additional paper if necessary) 2.
For the condition(s) requiring personal care: Americans with disabilities act complaint form (pdf) asbestos. Get your online template and fill it in using progressive features. Mds, dos, nps, pas, and specialist assistants. Share your form with others send doh 4359 via email, link, or fax. Patient identifying information (use additional paper if necessary) 2. Web doh form 4359 rating ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ 4.9 satisfied 373 votes how to fill out and sign doh form online? Follow the simple instructions below: Web required hiv related consent & authorization forms; Hiv/aids educational materials order forms;
Hiv/aids educational materials order forms; If the patient was examined bya physican’s assistant, specialist’s assistant, or nurse practioner, complete the required information(pg 1). Patient identifying information (use additional paper if necessary) 2. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Complete all items incomplete forms will be returned to the practitioner Web doh form 4359 rating ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ 4.9 satisfied 373 votes how to fill out and sign doh form online? For the condition(s) requiring personal care: Enjoy smart fillable fields and interactivity. Practitioners able to sign the nyia po forms include the following provider types: Edit your doh 4359 template online type text, add images, blackout confidential details, add comments, highlights and more.

Doh 1013 Form Fill Online, Printable, Fillable, Blank pdfFiller
Get your online template and fill it in using progressive features. Expanded syringe access program (esap) forms; Americans with disabilities act complaint form (pdf) asbestos. Complete all items incomplete forms will be returned to the practitioner Share your form with others send doh 4359 via email, link, or fax.

Tn Nashville Fill Online, Printable, Fillable, Blank pdfFiller
Expanded syringe access program (esap) forms; Hiv/aids educational materials order forms; Share your form with others send doh 4359 via email, link, or fax. Sign it in a few clicks draw your signature, type it, upload its image, or use your mobile device as a signature pad. Patient identifying information (use additional paper if necessary) 2.
Captain D's Application Pdf Fill Out and Sign Printable PDF Template
Expanded syringe access program (esap) forms; Hiv/aids educational materials order forms; Americans with disabilities act complaint form (pdf) asbestos. Mds, dos, nps, pas, and specialist assistants. Web required hiv related consent & authorization forms;

Doh 4359 form Fill out & sign online DocHub
Practitioners able to sign the nyia po forms include the following provider types: Expanded syringe access program (esap) forms; Hiv/aids educational materials order forms; Enjoy smart fillable fields and interactivity. Patient identifying information (use additional paper if necessary) 2.
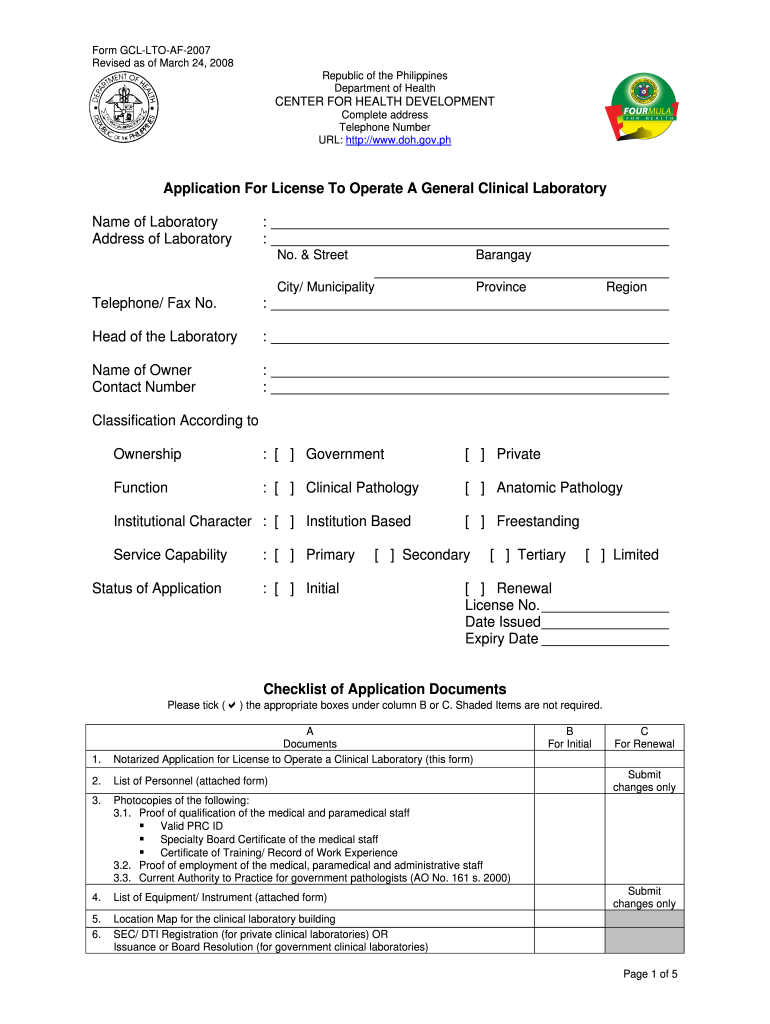
Doh Application Form for Renewal of License to Operate Fill Out and
Americans with disabilities act complaint form (pdf) asbestos. Share your form with others send doh 4359 via email, link, or fax. Get your online template and fill it in using progressive features. Patient identifying information (use additional paper if necessary) 2. Practitioners able to sign the nyia po forms include the following provider types:
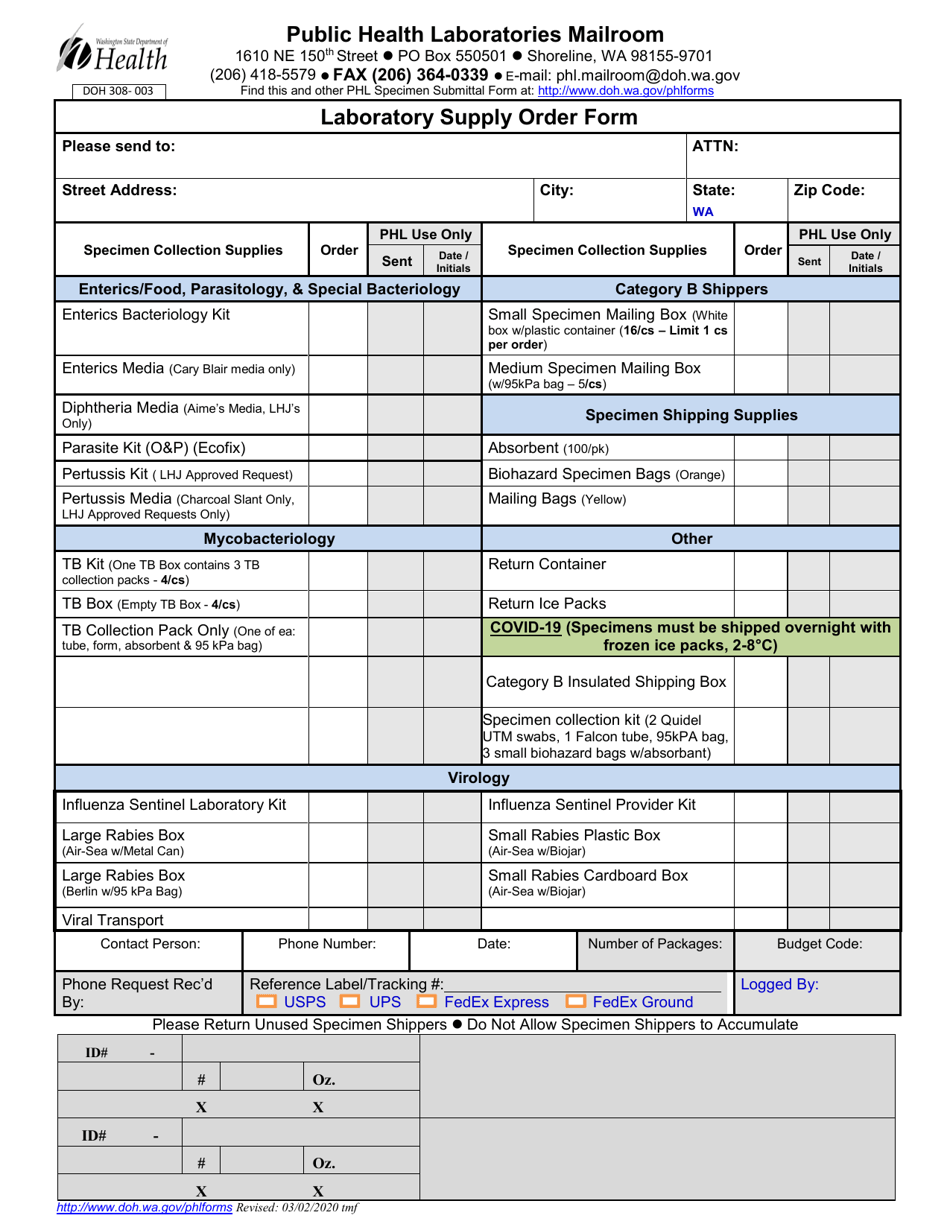
DOH Form 308003 Download Printable PDF or Fill Online Laboratory
The name, license number, and the complete business address must be indicated. Enjoy smart fillable fields and interactivity. Patient identifying information (use additional paper if necessary) 2. Web doh form 4359 rating ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ 4.9 satisfied 373 votes how to fill out and sign doh form online?.

600569 UK Doherty Baxter Cycle
Enjoy smart fillable fields and interactivity. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Complete all items incomplete forms will be returned to the practitioner Hiv/aids educational materials order forms; Patient identifying information (use additional paper if necessary) 2.
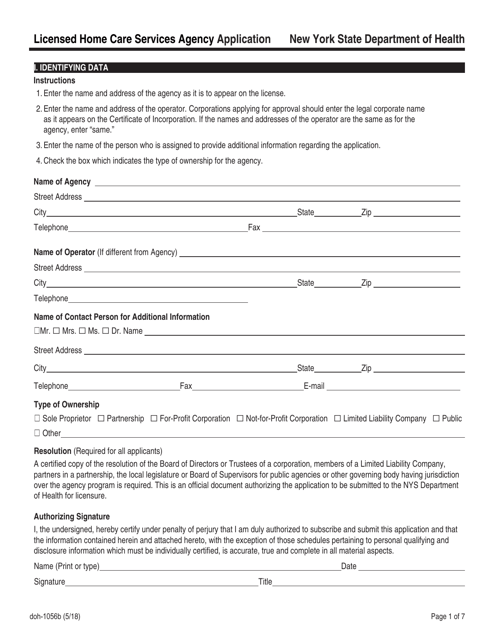
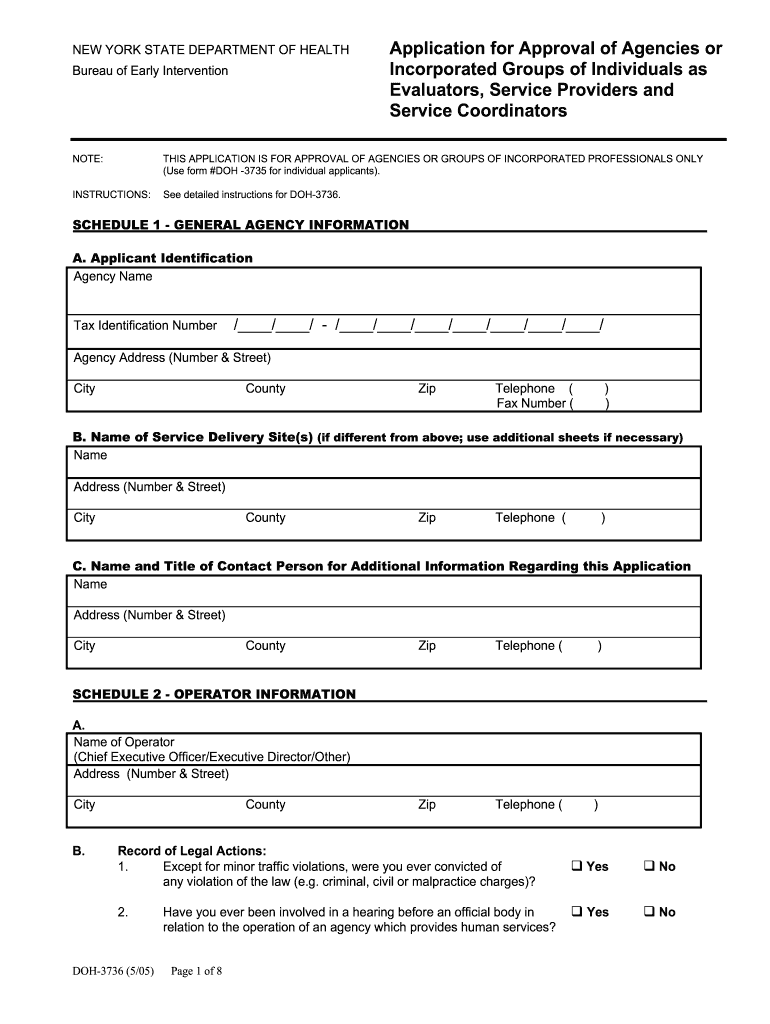
Form DOH1056B Download Fillable PDF or Fill Online Licensed Home Care
The name, license number, and the complete business address must be indicated. Americans with disabilities act complaint form (pdf) asbestos. Get your online template and fill it in using progressive features. Enjoy smart fillable fields and interactivity. Complete all items incomplete forms will be returned to the practitioner
Form DOH5131 Download Fillable PDF or Fill Online Funding Document for
Americans with disabilities act complaint form (pdf) asbestos. Patient identifying information (use additional paper if necessary) 2. Expanded syringe access program (esap) forms; Complete all items incomplete forms will be returned to the practitioner Practitioners able to sign the nyia po forms include the following provider types:

20122021 Form NY DOH4329 Fill Online, Printable, Fillable, Blank
For the condition(s) requiring personal care: Mds, dos, nps, pas, and specialist assistants. Web required hiv related consent & authorization forms; Enjoy smart fillable fields and interactivity. Practitioners able to sign the nyia po forms include the following provider types:
The Name, License Number, And The Complete Business Address Must Be Indicated.
Patient identifying information (use additional paper if necessary) 2. Americans with disabilities act complaint form (pdf) asbestos. Complete all items incomplete forms will be returned to the practitioner Mds, dos, nps, pas, and specialist assistants.
Practitioners Able To Sign The Nyia Po Forms Include The Following Provider Types:
Sign it in a few clicks draw your signature, type it, upload its image, or use your mobile device as a signature pad. For the condition(s) requiring personal care: Patient identifying information (use additional paper if necessary) 2. Web doh form 4359 rating ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ ★ 4.9 satisfied 373 votes how to fill out and sign doh form online?
Indicate N/A If An Item Does Not Apply To This Patient Or Unk If The Requested Information Is Unknown To The Physician Signing This Form.
Follow the simple instructions below: Enjoy smart fillable fields and interactivity. Share your form with others send doh 4359 via email, link, or fax. Get your online template and fill it in using progressive features.
If The Patient Was Examined Bya Physican’s Assistant, Specialist’s Assistant, Or Nurse Practioner, Complete The Required Information(Pg 1).
Expanded syringe access program (esap) forms; Web required hiv related consent & authorization forms; Hiv/aids educational materials order forms; Edit your doh 4359 template online type text, add images, blackout confidential details, add comments, highlights and more.