Dental Claim Form Pdf
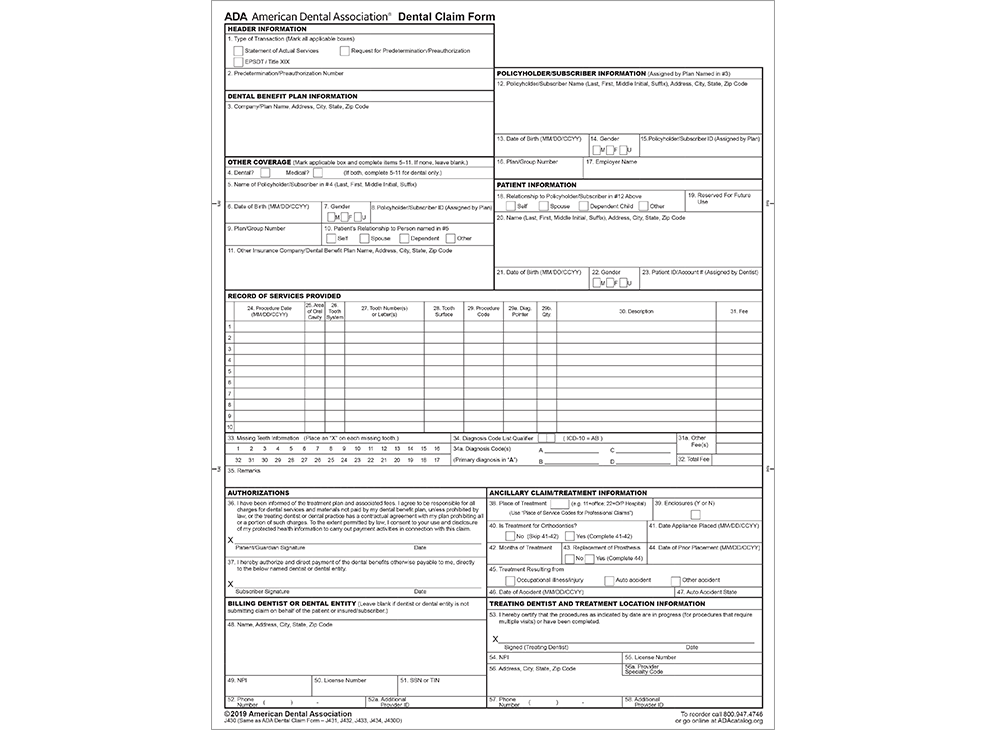
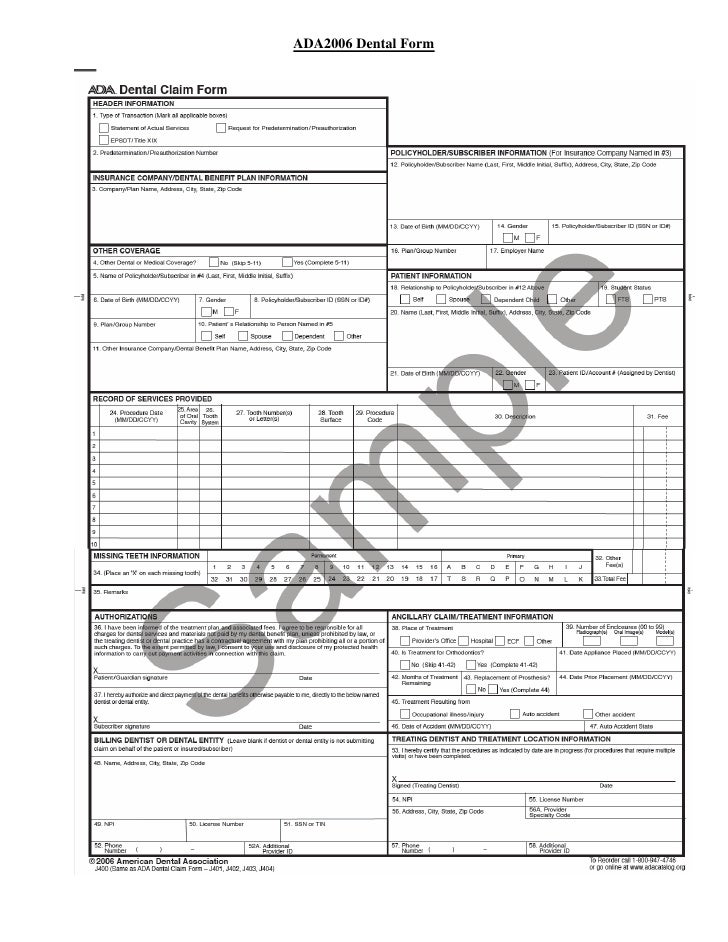
Dental Claim Form Pdf - Applications and forms for dentists and their patients. Relationship to primary subscriber (check applicable box) 19. Dental form back.pdf created date: Web this version of the ada form incorporates editorial changes to further its consistency with the 837d. Please download your copy of the ada 2019 claim form and start using this version immediately. This information is required when the diagnosis may affect claim adjudication when specific dental procedures may minimize the risks associated with. Company/plan name, address, city, state, zip code Any person who knowingly presents a false or fraudulent claim for payment for a. Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into the now current version of the hipaa standard (837d v5010) electronic dental claim. You or your designated representative is entitled to receive a copy of this claim form.
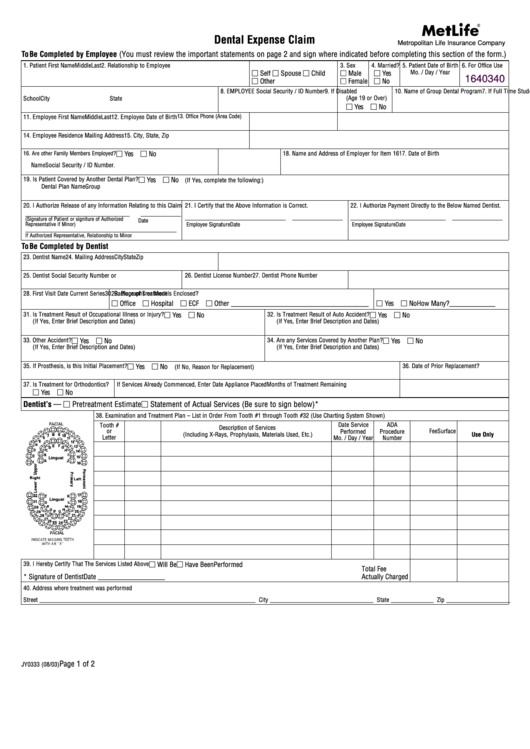
Complete all information requested below. Policyholder/subscriber name (last, first, middle initial, sufix), address, city, state, zip code 13. Web dental claim form 1. Date of birth (mm/dd/ccyy) 14. Applications and forms for dentists and their patients. Web the form supports reporting up to four diagnosis codes per dental procedure. Web plan start date / / patient’s name address patient’s date of birth / / is the patient under the age of 16? Web this version of the ada form incorporates editorial changes to further its consistency with the 837d. Use separate form for each family member and for each accident or illness. Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into the now current version of the hipaa standard (837d v5010) electronic dental claim.
Complete all information requested below. Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into the now current version of the hipaa standard (837d v5010) electronic dental claim. Date of birth (mm/dd/ccyy) 14. You or your designated representative is entitled to receive a copy of this claim form. Web this version of the ada form incorporates editorial changes to further its consistency with the 837d. Claim on behalf of the patient or insured/subscriber) patient information 18. Please download your copy of the ada 2019 claim form and start using this version immediately. This information is required when the diagnosis may affect claim adjudication when specific dental procedures may minimize the risks associated with. Web the ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. Lead member’s name phone number email address m m
Dental Claim Form, downloadable PDF ADA J430D
Ada policy promotes use and acceptance of the most current version of the ada dental claim form by dentists and payers. Web plan start date / / patient’s name address patient’s date of birth / / is the patient under the age of 16? Use separate form for each family member and for each accident or illness. Web dental claim.
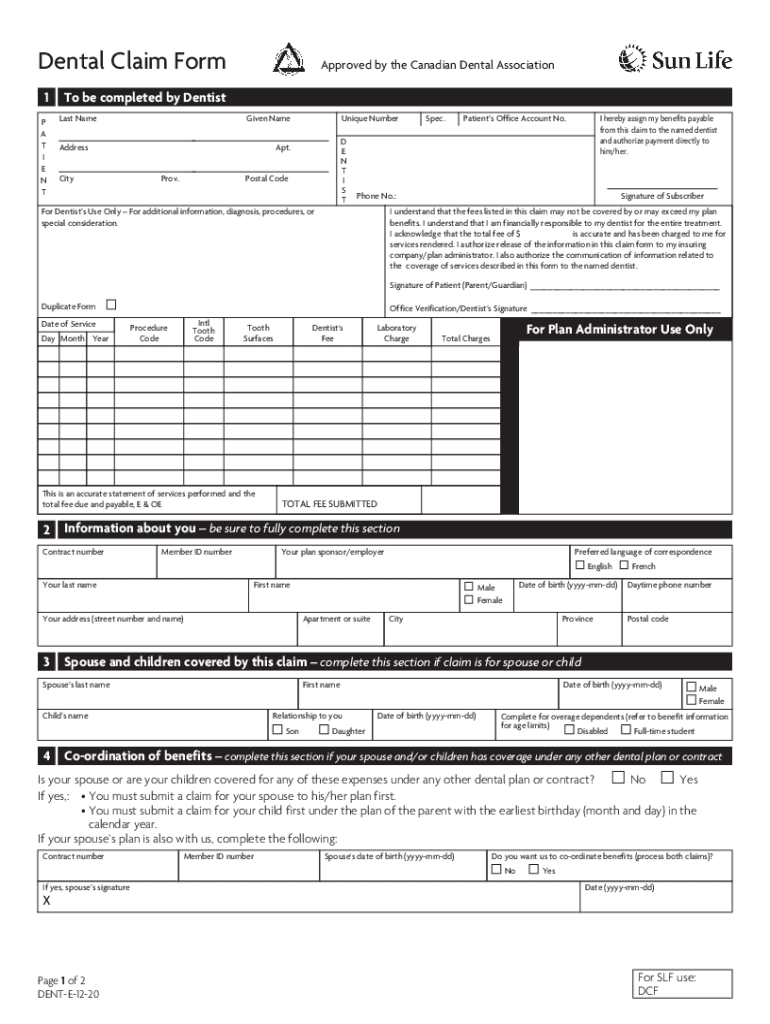
Sunlife Dental Claim Fill Out and Sign Printable PDF Template signNow
Lead member’s name phone number email address m m Policyholder/subscriber name (last, first, middle initial, sufix), address, city, state, zip code 13. Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into the now current version of the hipaa standard (837d v5010).
Dental Claim Form
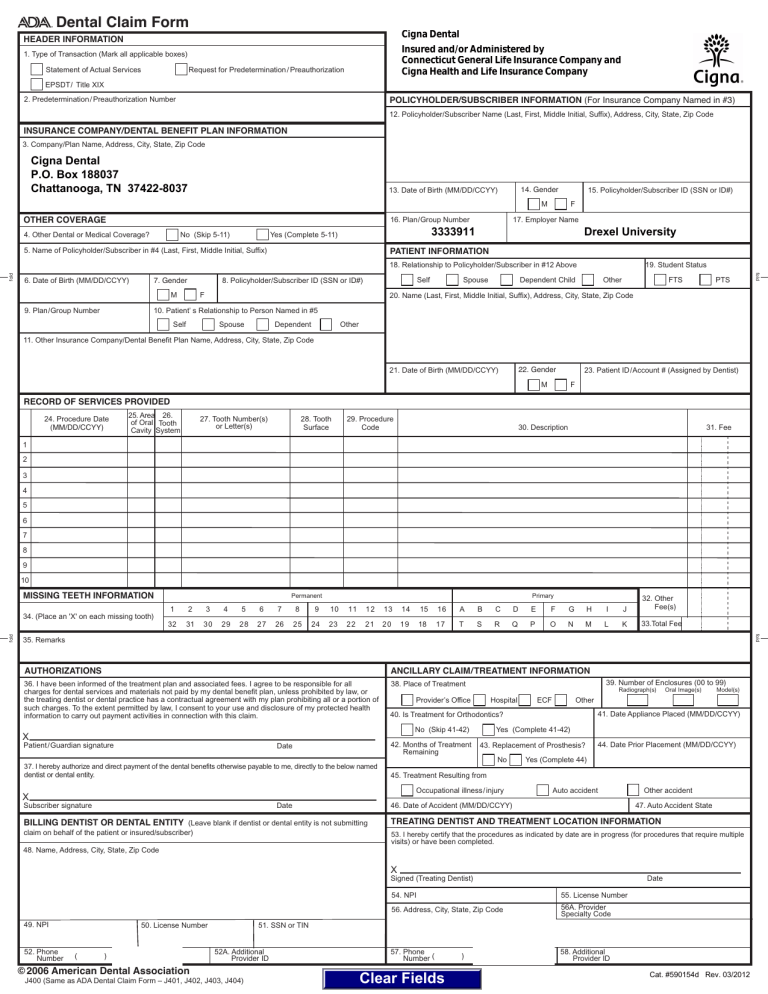
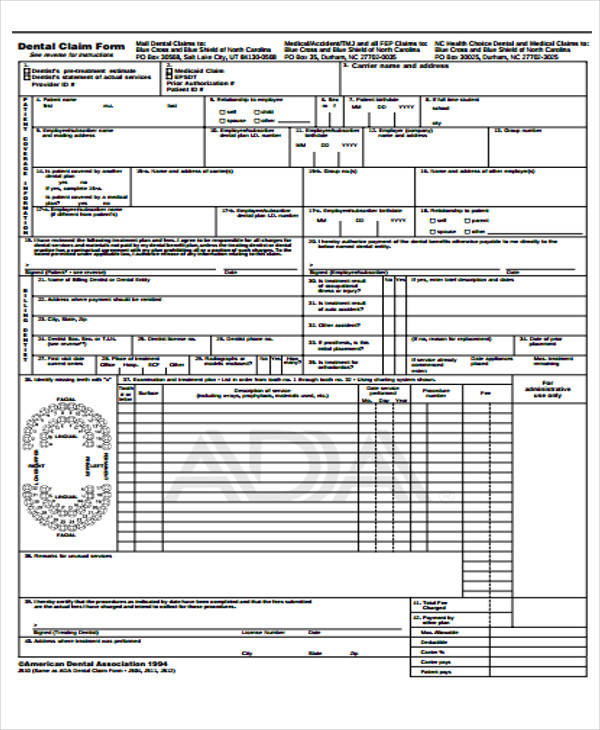
Company/plan name, address, city, state, zip code Web the ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. Web plan start date / / patient’s name address patient’s date of birth / / is the patient under the age of 16? Web dental claim form header information type of transaction (mark.
FREE 49+ Claim Forms in PDF
Applications and forms for dentists and their patients. Web dental claim form 1. Claim on behalf of the patient or insured/subscriber) patient information 18. This information is required when the diagnosis may affect claim adjudication when specific dental procedures may minimize the risks associated with. Complete all information requested below.
Dental Claim Form printable pdf download
Complete all information requested below. Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into the now current version of the hipaa standard (837d v5010) electronic dental claim. Web plan start date / / patient’s name address patient’s date of birth /.
FREE 31+ Claim Forms in MS Word
Web the form supports reporting up to four diagnosis codes per dental procedure. Web dental benefits claim form instructions 1. Date of birth (mm/dd/ccyy) 14. Claim on behalf of the patient or insured/subscriber) patient information 18. Relationship to primary subscriber (check applicable box) 19.

Prescription Form Template Online 123 Form Builder
Web the form supports reporting up to four diagnosis codes per dental procedure. Applications and forms for dentists and their patients. The following materials are prepared by ada practice institute staff with contributions from the ada council. Ada policy promotes use and acceptance of the most current version of the ada dental claim form by dentists and payers. Complete all.
Dental Claim Form
The following materials are prepared by ada practice institute staff with contributions from the ada council. Type of transaction (check all applicable boxes). Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into the now current version of the hipaa standard (837d.
Dental Insurance Claim Form Pdf
Web dental benefits claim form instructions 1. Policyholder/subscriber name (last, first, middle initial, sufix), address, city, state, zip code 13. Company/plan name, address, city, state, zip code Web dental claim form 1. Any person who knowingly presents a false or fraudulent claim for payment for a.
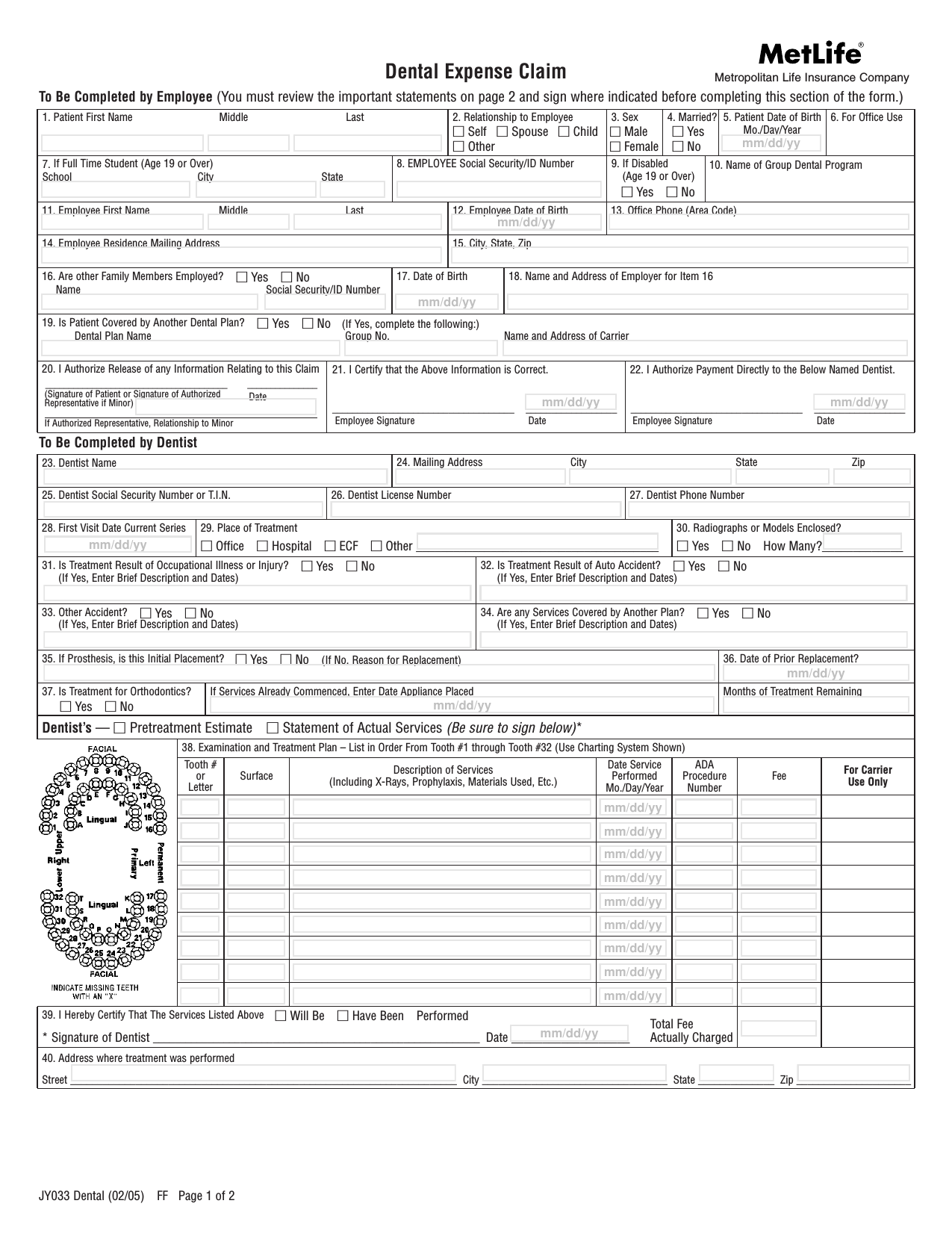
Download MetLife Dental Claim Form PDF
Web dental claim form header information type of transaction (mark all applicable boxes) statement of actual services request for predetermination/preauthorization epsdt / title xix predetermination/preauthorization number dental benefit plan information 3. Web the ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. If none, leave blank.) 4. Policyholder/subscriber name (last, first,.
Web Dental Claim Form Header Information Type Of Transaction (Mark All Applicable Boxes) Statement Of Actual Services Request For Predetermination/Preauthorization Epsdt / Title Xix Predetermination/Preauthorization Number Dental Benefit Plan Information 3.
Ada policy promotes use and acceptance of the most current version of the ada dental claim form by dentists and payers. Policyholder/subscriber name (last, first, middle initial, sufix), address, city, state, zip code 13. Web dental claim form 1. Company/plan name, address, city, state, zip code
Claim On Behalf Of The Patient Or Insured/Subscriber) Patient Information 18.
Complete all information requested below. Date of birth (mm/dd/ccyy) 14. Web plan start date / / patient’s name address patient’s date of birth / / is the patient under the age of 16? Web dental benefits claim form instructions 1.
If None, Leave Blank.) 4.
Applications and forms for dentists and their patients. Web the ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. Dental form back.pdf created date: Type of transaction (check all applicable boxes).
You Or Your Designated Representative Is Entitled To Receive A Copy Of This Claim Form.
Web the form supports reporting up to four diagnosis codes per dental procedure. Relationship to primary subscriber (check applicable box) 19. Use separate form for each family member and for each accident or illness. Any person who knowingly presents a false or fraudulent claim for payment for a.