Davis Vision Out Of Network Form
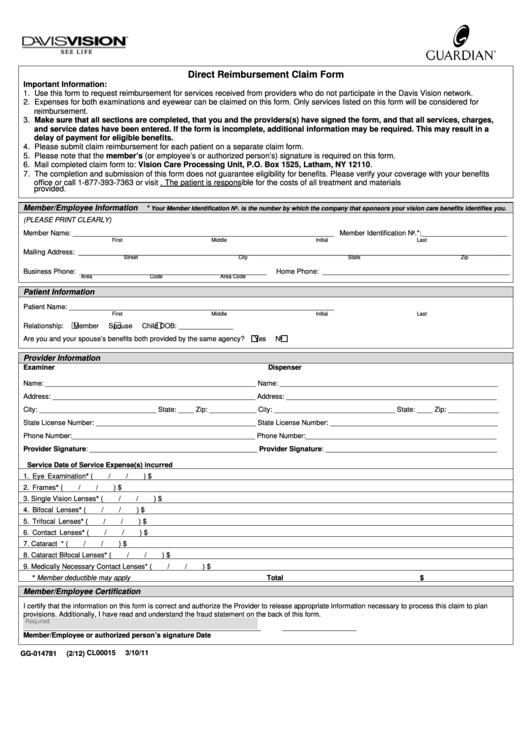
Davis Vision Out Of Network Form - Box 30978 salt lake city, ut 84130 fill in and sign the following form. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Vision care processing unit p.o. Web form instructions the form must be filled out by the member. Expenses for both examinations and eyewear can be claimed on this. Only one patient’s services may be claimed on this form. Fill it out on a computer, print it, and mail it in. All fields flagged with an asterisk (*) are required. Select the patient’s relation to the member. Expenses for both examinations and eyewear can be listed on this form.
Each patient’s services must be claimed on a separate form. Use this form to request reimbursement for services received from providers not in the davis vision network. Box 1525 latham, ny 12110 united healthcare vision (spectera) attn: Includes dilation when professionally indicated. Expenses for both examinations and eyewear can be claimed on this form. Expenses for both examinations and eyewear can be claimed on this form. Box 30978 salt lake city, ut 84130 fill in and sign the following form. Expenses for both examinations and eyewear can be listed on this form. Attach an itemized receipt to the form. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network.
Fill it out on a computer, print it, and mail it in. Each patient’s services must be claimed on a separate form. All fields flagged with an asterisk (*) are required. Attach an itemized receipt to the form. Expenses for both examinations and eyewear can be claimed on this form. The form is fillable, so you do not have to hand write. Use this form to request reimbursement for services received from providers not in the davis vision network. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Available in all ranges of prescriptions and sizes with tinting and scratch resistant coating frame12 months Box 30978 salt lake city, ut 84130 fill in and sign the following form.

Davis Vision "Out of Network" claim form by Drs. Stahl & Calder Issuu
Expenses for both examinations and eyewear can be claimed on this form. Box 1525 latham, ny 12110 united healthcare vision (spectera) attn: Expenses for both examinations and eyewear can be claimed on this form. Available in all ranges of prescriptions and sizes with tinting and scratch resistant coating frame12 months Expenses for both examinations and eyewear can be claimed on.
Top Davis Vision Claim Form Templates free to download in PDF format
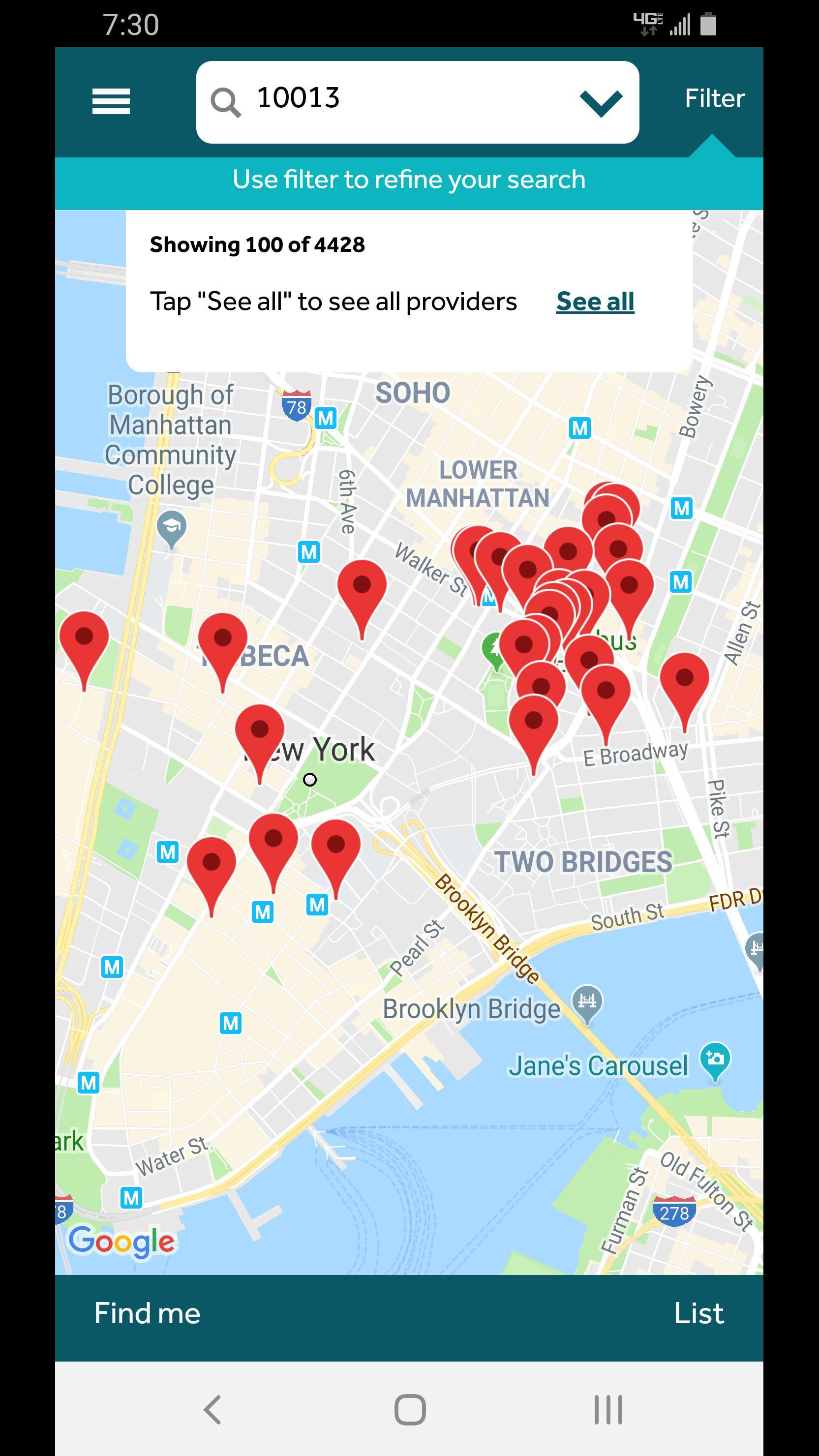
Log in to your account and click on “access benefits and forms” to download the direct reimbursement claim form. Select the patient’s relation to the member. Only one patient’s services may be claimed on this form. Fill it out on a computer, print it, and mail it in. Box 1525 latham, ny 12110 united healthcare vision (spectera) attn:

Davis Vision "Out of Network" claim form by Drs. Stahl & Calder Issuu
Expenses for both examinations and eyewear can be claimed on this form. Vision care processing unit p.o. Fill it out on a computer, print it, and mail it in. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Select the patient’s relation to the member.

Davis Vision Insurance Plans Davis Vision 10 40 Off S Blue365 Deals
Available in all ranges of prescriptions and sizes with tinting and scratch resistant coating frame12 months Expenses for both examinations and eyewear can be claimed on this form. If you decide to hand write, use blue or black ink. Includes dilation when professionally indicated. Expenses for both examinations and eyewear can be claimed on this form.

Davis Vision Insurance Providers In My Area Does Costco Accept Davis
If you decide to hand write, use blue or black ink. Box 30978 salt lake city, ut 84130 fill in and sign the following form. Vision care processing unit p.o. Select the patient’s relation to the member. Expenses for both examinations and eyewear can be claimed on this form.

Davis Vision Insurance Providers In My Area Does Costco Accept Davis
Log in to your account and click on “access benefits and forms” to download the direct reimbursement claim form. The form is fillable, so you do not have to hand write. Available in all ranges of prescriptions and sizes with tinting and scratch resistant coating frame12 months Attach an itemized receipt to the form. Web vision service plan (vsp) attn:

davis vision Texas Vision Clinic
Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Fill it out on a computer, print it, and mail it in. Includes dilation when professionally indicated. Use this form to request reimbursement for services received from providers not in the davis vision network. Only one patient’s services may.
Davis Vision for Android APK Download
Includes dilation when professionally indicated. Box 30978 salt lake city, ut 84130 fill in and sign the following form. Expenses for both examinations and eyewear can be claimed on this. Use this form to request reimbursement for services received from providers not in the davis vision network. Expenses for both examinations and eyewear can be claimed on this form.
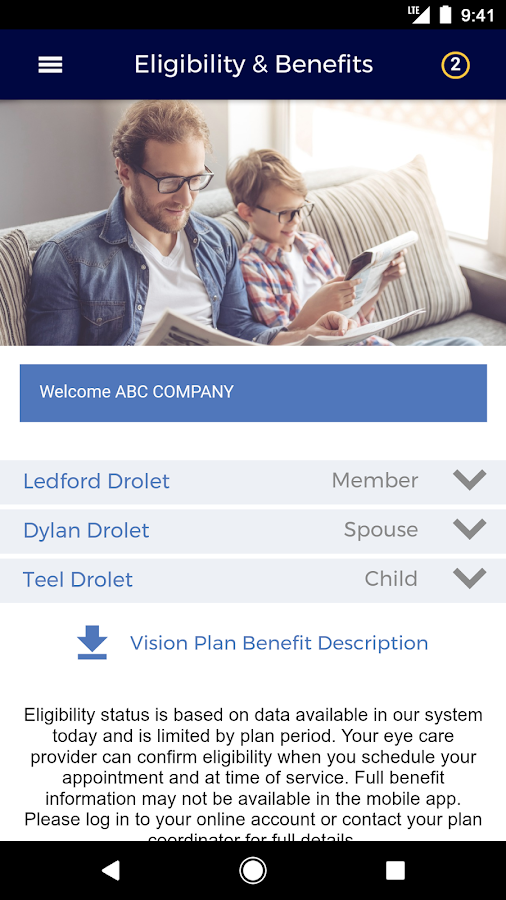
Davis Vision Android Apps on Google Play
Expenses for both examinations and eyewear can be claimed on this. If you decide to hand write, use blue or black ink. Log in to your account and click on “access benefits and forms” to download the direct reimbursement claim form. The form is fillable, so you do not have to hand write. Includes dilation when professionally indicated.
:max_bytes(150000):strip_icc()/davis-vision-e1058df5c44c46dc966fb0bba20f3086.jpg)
Best Vision Insurance Companies of 2022
Fill it out on a computer, print it, and mail it in. Expenses for both examinations and eyewear can be claimed on this form. Includes dilation when professionally indicated. Select the patient’s relation to the member. The form is fillable, so you do not have to hand write.
Use This Form To Request Reimbursement For Services Received From Providers Not In The Davis Vision Network.
Box 1525 latham, ny 12110 united healthcare vision (spectera) attn: Expenses for both examinations and eyewear can be listed on this form. Each patient’s services must be claimed on a separate form. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network.
Box 30978 Salt Lake City, Ut 84130 Fill In And Sign The Following Form.
Available in all ranges of prescriptions and sizes with tinting and scratch resistant coating frame12 months Expenses for both examinations and eyewear can be claimed on this. Expenses for both examinations and eyewear can be claimed on this form. Web vision service plan (vsp) attn:
The Form Is Fillable, So You Do Not Have To Hand Write.
Includes dilation when professionally indicated. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. All fields flagged with an asterisk (*) are required. Expenses for both examinations and eyewear can be claimed on this form.
Log In To Your Account And Click On “Access Benefits And Forms” To Download The Direct Reimbursement Claim Form.
Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Only one patient’s services may be claimed on this form. Web form instructions the form must be filled out by the member. Select the patient’s relation to the member.