Cvs Caremark Medication Prior Auth Form
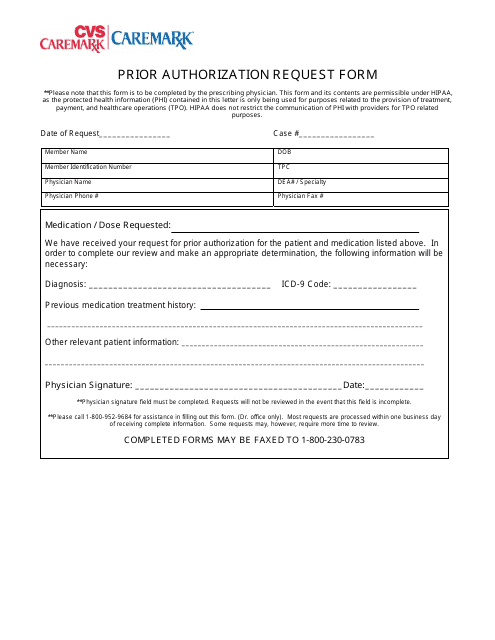
Cvs Caremark Medication Prior Auth Form - Coverage criteria the requested drug will be covered with prior. Web we offer access to specialty medications and infusion therapies, centralized intake and benefits verification, and prior authorization assistance. Please fill out all applicable sections. Web request for medicare prescription drug coverage determination this form may be sent to us by mail or fax: Select the starting letter of the name of the medication to begin. Web select the appropriate cvs caremark form to get started. Covermymeds is cvs caremark prior authorization forms’s preferred method for receiving epa requests. Web pharmaceutical manufacturers not affiliated with cvs caremark. Web i attest that the medication requested is medically necessary for this patient. Through their ongoing collaboration, cvs caremark and surescripts have partnered to provide free epa.
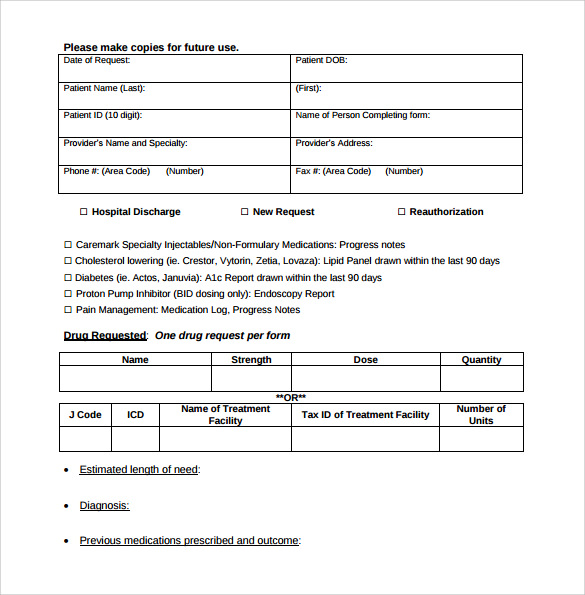
Select the starting letter of the name of the medication to begin. Web all you need to do is to pick the cvs caremark prior authorization form pdf, complete the needed areas, include fillable fields (if necessary), and sign it without having second. Web prior authorization criteria drug class weight loss management brand name (generic) contrave (naltrexone hcl and bupropion hcl extended. Coverage criteria the requested drug will be covered with prior. Web prior authorization requests for drugs covered under the medical benefit must be submitted electronically through the carefirst provider portal. Web pharmaceutical manufacturers not affiliated with cvs caremark. Through their ongoing collaboration, cvs caremark and surescripts have partnered to provide free epa. Web submit electronic prior authorization requests free secure easy. Web we offer access to specialty medications and infusion therapies, centralized intake and benefits verification, and prior authorization assistance. Web prescription drug prior authorization or step therapy exception request form patient name:
Select the starting letter of the name of the medication to begin. Web prior authorization criteria drug class weight loss management brand name (generic) contrave (naltrexone hcl and bupropion hcl extended. Covermymeds is cvs caremark prior authorization forms’s preferred method for receiving epa requests. Web i attest that the medication requested is medically necessary for this patient. Web we offer access to specialty medications and infusion therapies, centralized intake and benefits verification, and prior authorization assistance. Coverage criteria the requested drug will be covered with prior. I further attest that the information provided is accurate and true, and that documentation supporting. Web prescription drug prior authorization or step therapy exception request form patient name: Web pharmaceutical manufacturers not affiliated with cvs caremark. Web prior authorization requests for drugs covered under the medical benefit must be submitted electronically through the carefirst provider portal.
FREE 8+ Sample Prior Authorization Forms in PDF MS Word
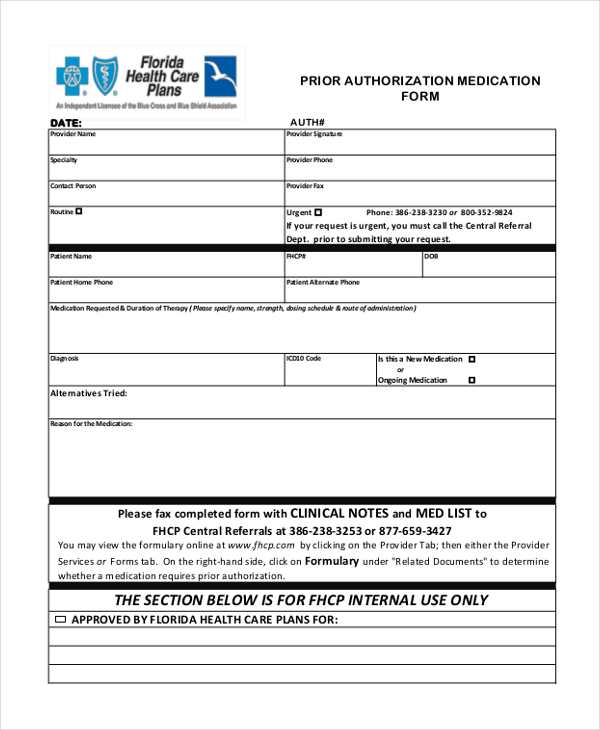
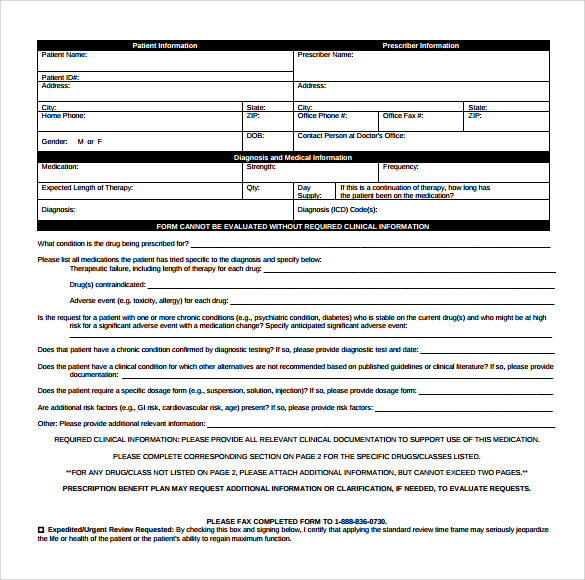
I further attest that the information provided is accurate and true, and that documentation supporting. Through their ongoing collaboration, cvs caremark and surescripts have partnered to provide free epa. Web download, review and print the prior approval form for the requested medication. Web prescription drug prior authorization or step therapy exception request form patient name: Prior authorization requests must be.
Prior Authorization Request Form Cvs Caremark Download Printable PDF
Use the arrows next to each. To submit a prior authorization. Web pharmaceutical manufacturers not affiliated with cvs caremark. Select the starting letter of the name of the medication to begin. Coverage criteria the requested drug will be covered with prior.
Template Caremark Prior Authorization Form Mous Syusa
To submit a prior authorization. Web request for medicare prescription drug coverage determination this form may be sent to us by mail or fax: Web pharmaceutical manufacturers not affiliated with cvs caremark. Prior authorization requests must be submitted electronically through the carefirst provider portal for all drugs requiring prior authorization. 711), 24 hours a day, 7 days a week, or.
FREE 8+ Sample Caremark Prior Authorization Forms in PDF
Web submit electronic prior authorization requests free secure easy. Web prescription drug prior authorization or step therapy exception request form patient name: Web i attest that the medication requested is medically necessary for this patient. Web prior authorization requests for drugs covered under the medical benefit must be submitted electronically through the carefirst provider portal. Web request for medicare prescription.
Sample Caremark Prior Authorization Form 8+ Free Documents in PDF
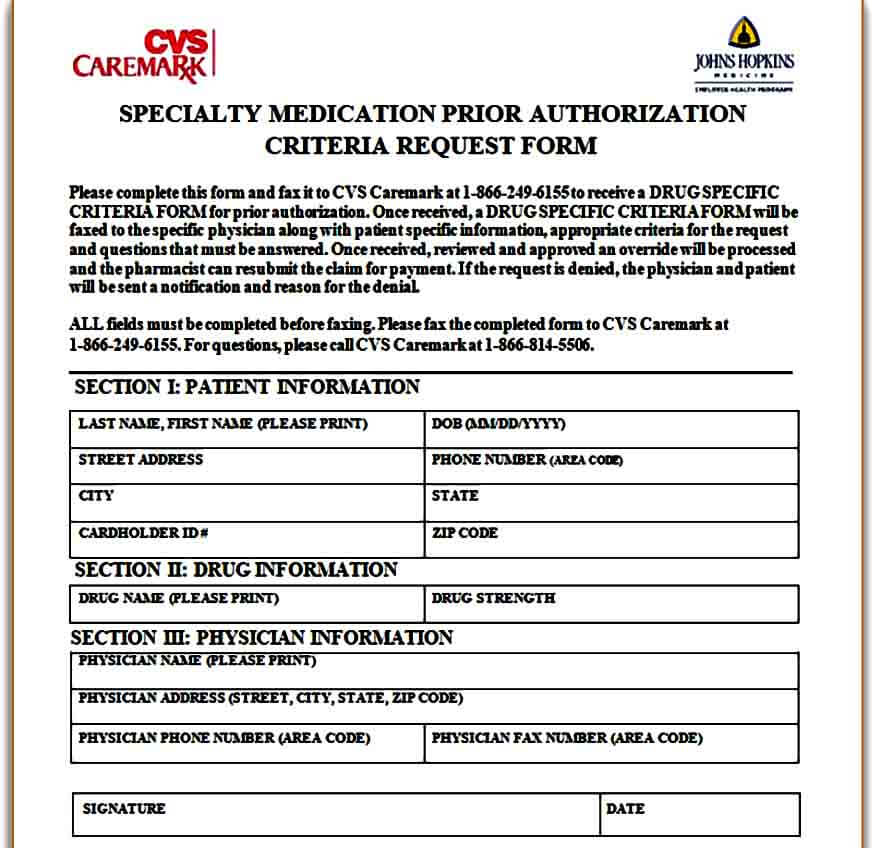
Covermymeds is cvs caremark prior authorization forms’s preferred method for receiving epa requests. Web i attest that the medication requested is medically necessary for this patient. Web submit electronic prior authorization requests free secure easy. Web select the appropriate cvs caremark form to get started. Please fill out all applicable sections.
FREE 8+ Sample Caremark Prior Authorization Forms in PDF
Use the arrows next to each. Prior authorization requests must be submitted electronically through the carefirst provider portal for all drugs requiring prior authorization. Coverage criteria the requested drug will be covered with prior. Covermymeds is cvs caremark prior authorization forms’s preferred method for receiving epa requests. Web prior authorization criteria drug class weight loss management brand name (generic) contrave.
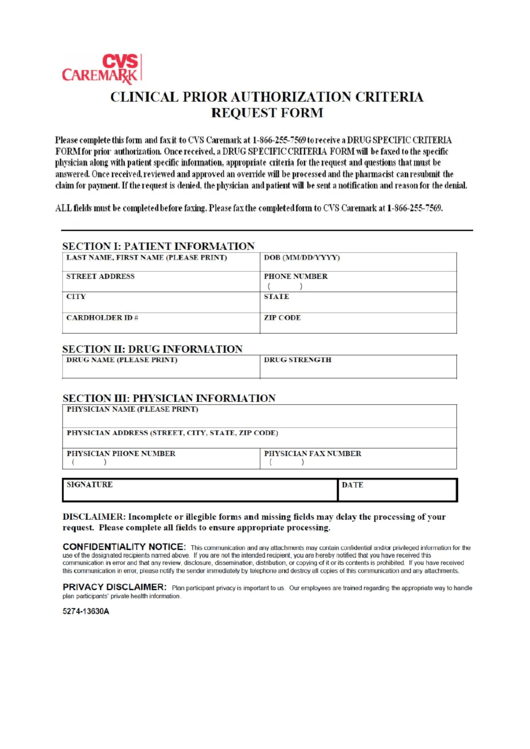
Caremark Prior Authorization Criteria Request Form printable pdf download
Prior authorization requests must be submitted electronically through the carefirst provider portal for all drugs requiring prior authorization. To submit a prior authorization. Web submit electronic prior authorization requests free secure easy. Web request for medicare prescription drug coverage determination this form may be sent to us by mail or fax: Select the starting letter of the name of the.

FastStart 10613946a Fill and Sign Printable Template Online US
Web all you need to do is to pick the cvs caremark prior authorization form pdf, complete the needed areas, include fillable fields (if necessary), and sign it without having second. Web prior authorization requests for drugs covered under the medical benefit must be submitted electronically through the carefirst provider portal. Please fill out all applicable sections. Web submit electronic.

CVS Caremark 10637207A 20192021 Fill and Sign Printable Template
Coverage criteria the requested drug will be covered with prior. To submit a prior authorization. Web prior authorization requests for drugs covered under the medical benefit must be submitted electronically through the carefirst provider portal. Web i attest that the medication requested is medically necessary for this patient. Web prescription drug prior authorization or step therapy exception request form patient.

Free CVS/Caremark Prior (Rx) Authorization Form PDF eForms
Web download, review and print the prior approval form for the requested medication. Web submit electronic prior authorization requests free secure easy. Web we offer access to specialty medications and infusion therapies, centralized intake and benefits verification, and prior authorization assistance. I further attest that the information provided is accurate and true, and that documentation supporting. Web prior authorization requests.
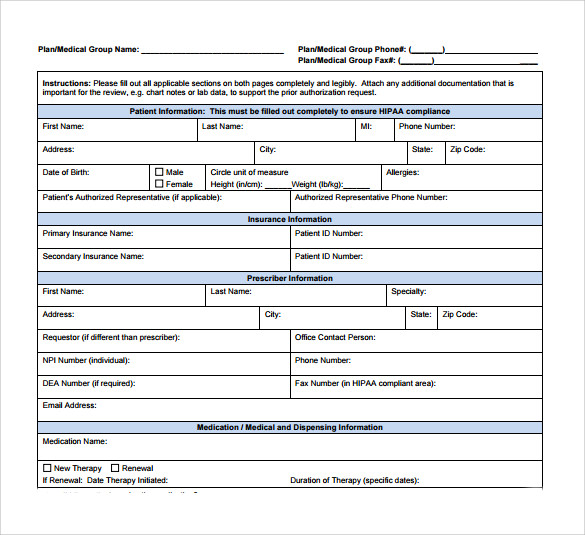
Please Fill Out All Applicable Sections.
Web all you need to do is to pick the cvs caremark prior authorization form pdf, complete the needed areas, include fillable fields (if necessary), and sign it without having second. Coverage criteria the requested drug will be covered with prior. Web prior authorization criteria drug class weight loss management brand name (generic) contrave (naltrexone hcl and bupropion hcl extended. Web prior authorization requests for drugs covered under the medical benefit must be submitted electronically through the carefirst provider portal.
Web I Attest That The Medication Requested Is Medically Necessary For This Patient.
Web prescription drug prior authorization or step therapy exception request form patient name: 711), 24 hours a day, 7 days a week, or through our website at. Covermymeds is cvs caremark prior authorization forms’s preferred method for receiving epa requests. Web submit electronic prior authorization requests free secure easy.
I Further Attest That The Information Provided Is Accurate And True, And That Documentation Supporting.
Through their ongoing collaboration, cvs caremark and surescripts have partnered to provide free epa. Web we offer access to specialty medications and infusion therapies, centralized intake and benefits verification, and prior authorization assistance. Web pharmaceutical manufacturers not affiliated with cvs caremark. Select the starting letter of the name of the medication to begin.
Web Download, Review And Print The Prior Approval Form For The Requested Medication.
Web request for medicare prescription drug coverage determination this form may be sent to us by mail or fax: Use the arrows next to each. Web select the appropriate cvs caremark form to get started. Prior authorization requests must be submitted electronically through the carefirst provider portal for all drugs requiring prior authorization.