Consent To Treat Minor Form
Consent To Treat Minor Form - This additional information will assist in treatment if it can be furnished with the consent but is not required. Web it is understood that this authorization is given to provide authority and power on the part of my aforesaid agent(s) to give specific consent to any and all such evaluation, diagnosis, office treatment, anesthetic administration or surgical treatment(s) which a physician, in the exercise of his/her best judgment, may deem advisable. This person must be 18 years of age or older. Web updated june 03, 2022. A copy of the authorization should be made a part of the minor's medical record. A minor (child) medical consent is a legal document providing someone other than the parent or legal guardian temporary rights to seek and provide healthcare and healthcare decisions on. I, (full name of parent or legal guardian) _____ Family address _____ father’s telephone: Minor child medical authorization form. Minors under the supervision of foster parents:
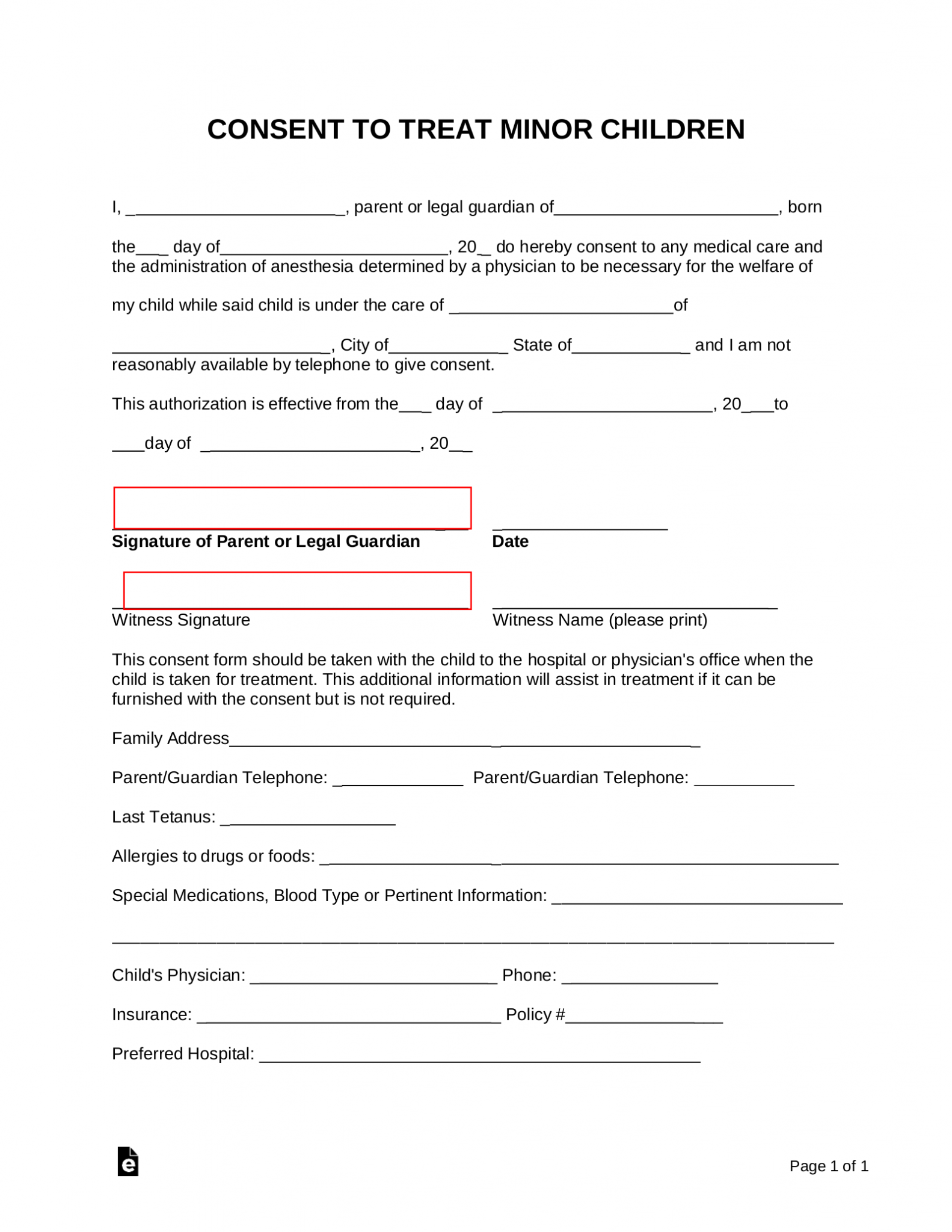
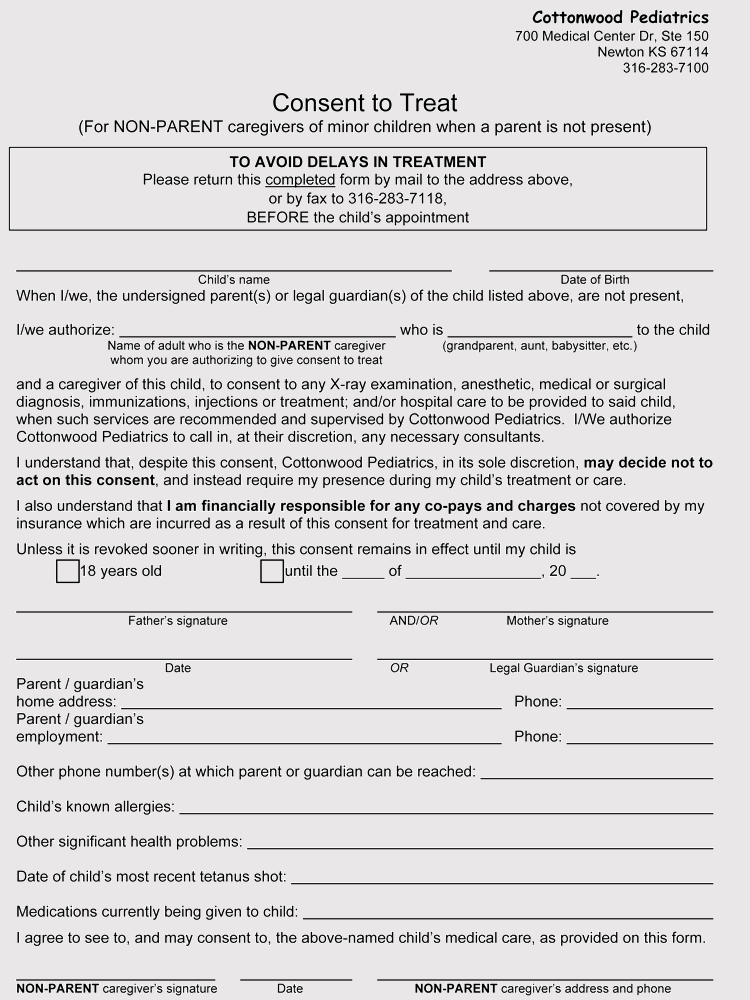
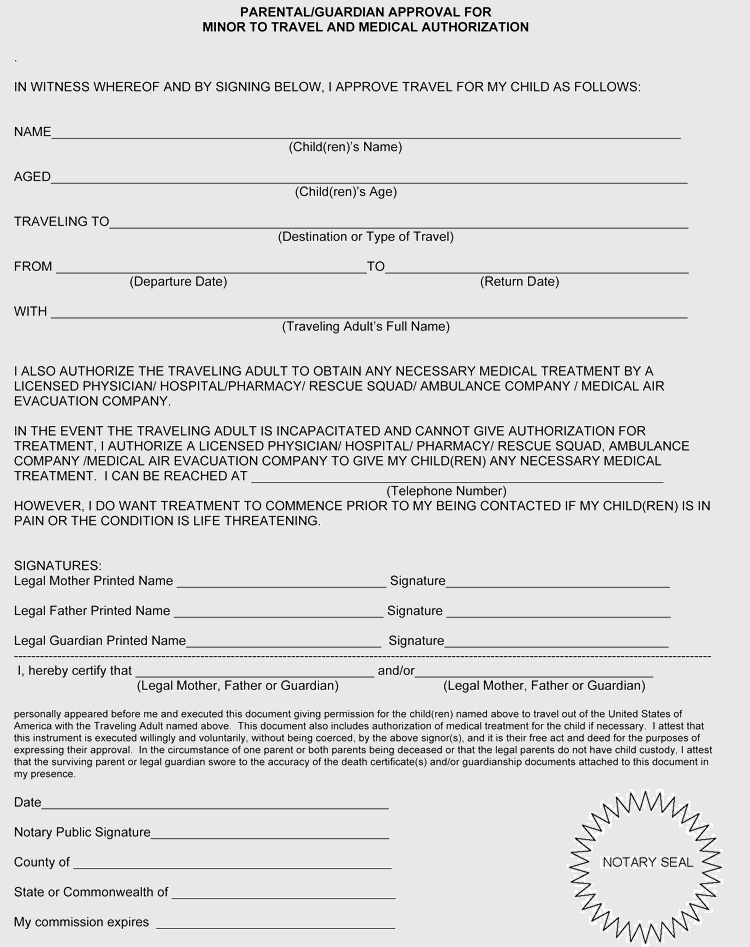
It is a simple one (1) page document that authorizes a third (3rd) party representative to handle any questions or requests by doctors or hospital staff in. This person must be 18 years of age or older. A minor (child) medical consent is a legal document providing someone other than the parent or legal guardian temporary rights to seek and provide healthcare and healthcare decisions on. Minor child medical authorization form. Web should your child need to be seen at nationwide children’s hospital, we must have your written consent to allow the person you select to seek treatment and sign the consent form. This additional information will assist in treatment if it can be furnished with the consent but is not required. Web consent to treat minor children i, _ _, parent or legal guardian of , born the _ day of , 20 _ do hereby consent to any medical care and the administration of anesthesia determined by a physician to be necessary for the welfare of my child while said child is under the care of _ I, (full name of parent or legal guardian) _____ Web it is understood that this authorization is given to provide authority and power on the part of my aforesaid agent(s) to give specific consent to any and all such evaluation, diagnosis, office treatment, anesthetic administration or surgical treatment(s) which a physician, in the exercise of his/her best judgment, may deem advisable. This additional information will assist in treatment if it can be furnished with the consent but is not required.
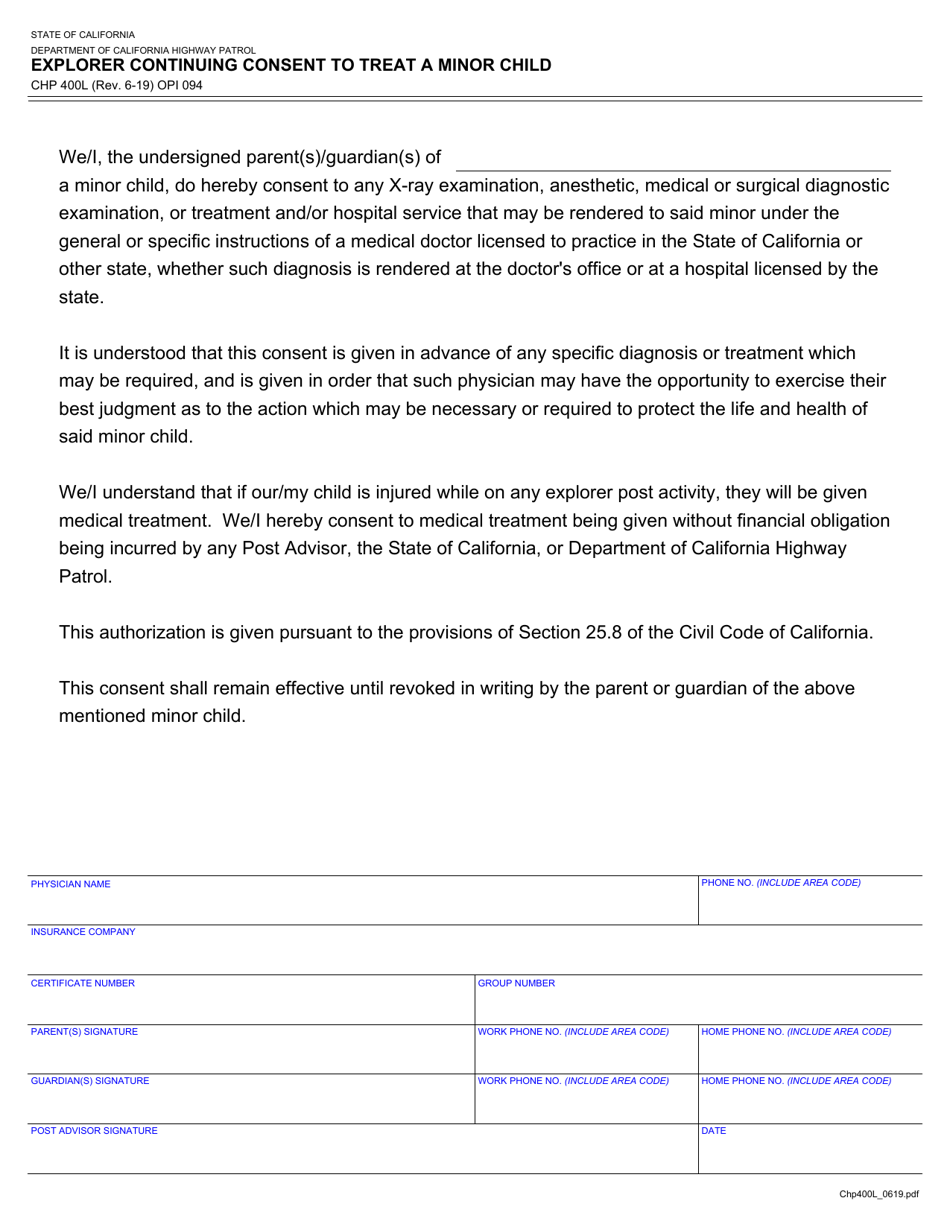
This additional information will assist in treatment if it can be furnished with the consent but is not required. I, (full name of parent or legal guardian) _____ Minor child medical authorization form. A copy of the authorization should be made a part of the minor's medical record. Web the simple form gives clear, irrefutable consent for medical treatment—until you can step in. Web it is understood that this authorization is given to provide authority and power on the part of my aforesaid agent(s) to give specific consent to any and all such evaluation, diagnosis, office treatment, anesthetic administration or surgical treatment(s) which a physician, in the exercise of his/her best judgment, may deem advisable. Minors under the supervision of foster parents: This additional information will assist in treatment if it can be furnished with the consent but is not required. Web this consent form should be taken with the child to the hospital or physician's office when the child is taken for treatment. A minor medical treatment authorization form allows a parent or guardian to select someone else to handle the primary health care decisions of their child.
Free Minor (Child) Medical Consent Form PDF Word eForms
Minors under the supervision of foster parents: Web should your child need to be seen at nationwide children’s hospital, we must have your written consent to allow the person you select to seek treatment and sign the consent form. This additional information will assist in treatment if it can be furnished with the consent but is not required. A minor.
Sample Letter For Permission To Treat Child For Your Needs Letter
Web this consent form should be taken with the child to the hospital or physician's office when the child is taken for treatment. This additional information will assist in treatment if it can be furnished with the consent but is not required. This person must be 18 years of age or older. Web updated june 03, 2022. I, (full name.
Printable Medical Consent Form For Minor While Parents Are Away Fill
Web this consent form should be taken with the child to the hospital or physician's office when the child is taken for treatment. Minor child medical authorization form. This person must be 18 years of age or older. This additional information will assist in treatment if it can be furnished with the consent but is not required. Web updated june.

Medical Treatment Authorization Fill Online, Printable, Fillable
Web the simple form gives clear, irrefutable consent for medical treatment—until you can step in. Minors under the supervision of foster parents: This person must be 18 years of age or older. Web consent to treat minor children i, _ _, parent or legal guardian of , born the _ day of , 20 _ do hereby consent to any.
Form CHP400L Download Fillable PDF or Fill Online Explorer Continuing
Web should your child need to be seen at nationwide children’s hospital, we must have your written consent to allow the person you select to seek treatment and sign the consent form. This additional information will assist in treatment if it can be furnished with the consent but is not required. Web this consent form should be taken with the.

Consent To Treat Form Fill Online, Printable, Fillable, Blank pdfFiller
Web should your child need to be seen at nationwide children’s hospital, we must have your written consent to allow the person you select to seek treatment and sign the consent form. Family address _____ father’s telephone: A copy of the authorization should be made a part of the minor's medical record. This additional information will assist in treatment if.
Ssurvivor Child Medical Consent Form
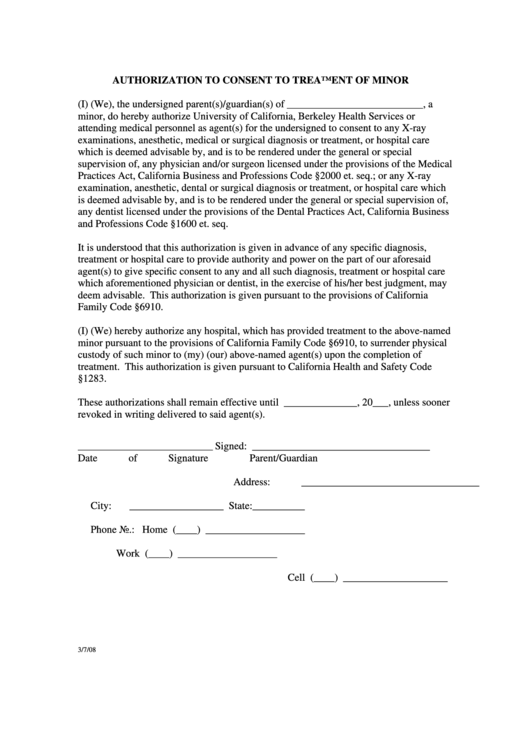
Web it is understood that this authorization is given to provide authority and power on the part of my aforesaid agent(s) to give specific consent to any and all such evaluation, diagnosis, office treatment, anesthetic administration or surgical treatment(s) which a physician, in the exercise of his/her best judgment, may deem advisable. This additional information will assist in treatment if.
Authorization To Consent To Treatment Of Minor Form printable pdf download
Web should your child need to be seen at nationwide children’s hospital, we must have your written consent to allow the person you select to seek treatment and sign the consent form. This additional information will assist in treatment if it can be furnished with the consent but is not required. Web it is understood that this authorization is given.
Consent For Medical Treatment Of A Minor Consent For Medical Treatment
Web consent to treat minor children i, _ _, parent or legal guardian of , born the _ day of , 20 _ do hereby consent to any medical care and the administration of anesthesia determined by a physician to be necessary for the welfare of my child while said child is under the care of _ Family address _____.
.jpg)
Have the Parents Signed an Authorization to Treat a Minor Consent Form?
This additional information will assist in treatment if it can be furnished with the consent but is not required. This person must be 18 years of age or older. A copy of the authorization should be made a part of the minor's medical record. I, (full name of parent or legal guardian) _____ A minor (child) medical consent is a.
Web Consent To Treat Minor Children I, _ _, Parent Or Legal Guardian Of , Born The _ Day Of , 20 _ Do Hereby Consent To Any Medical Care And The Administration Of Anesthesia Determined By A Physician To Be Necessary For The Welfare Of My Child While Said Child Is Under The Care Of _
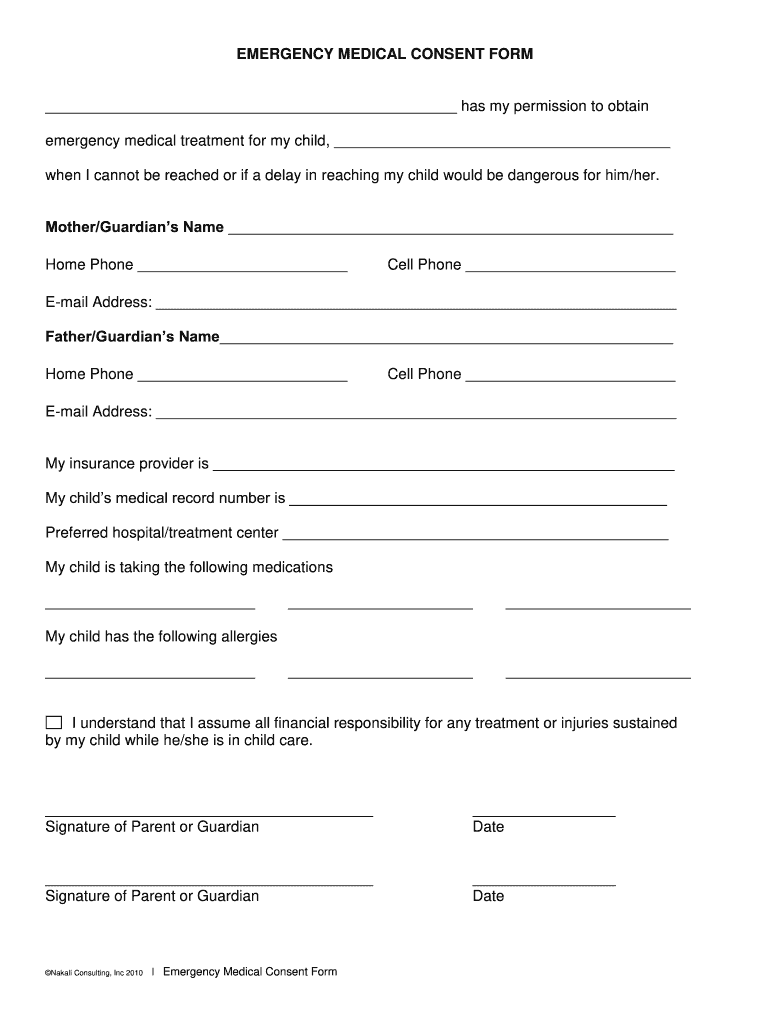
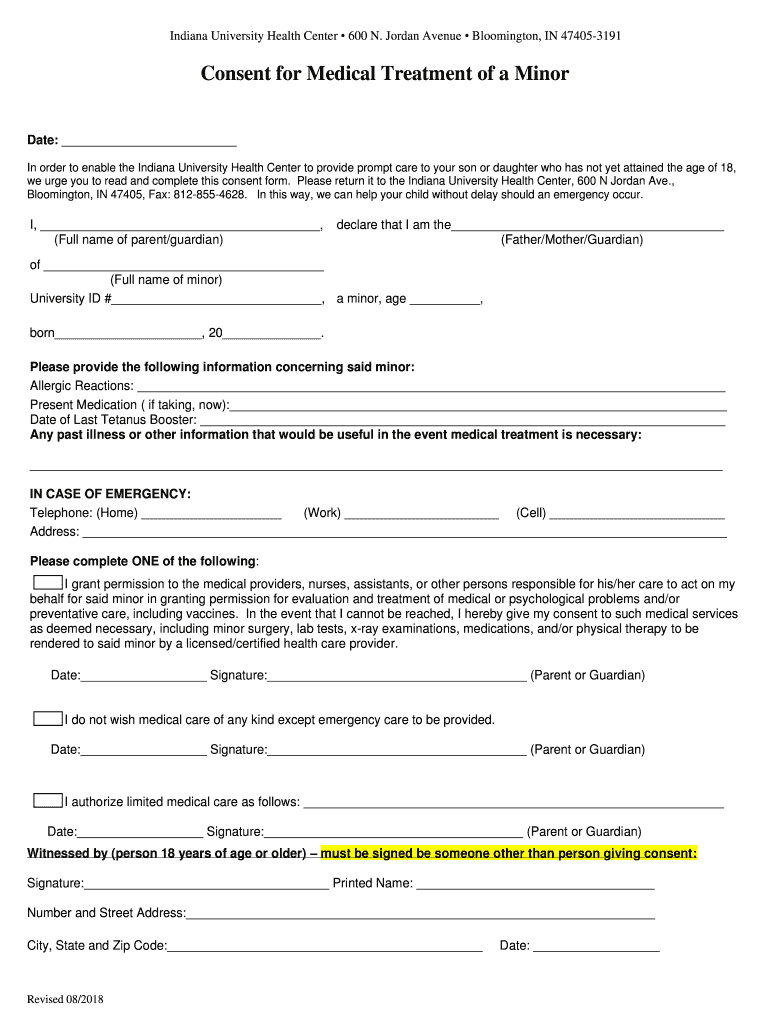
This additional information will assist in treatment if it can be furnished with the consent but is not required. Minor child medical authorization form. This makes it possible for your child to get immediate care even if they are not with you, like if they break a bone while with the babysitter or at daycare, or have an allergic reaction while staying with grandma, for example. A minor (child) medical consent is a legal document providing someone other than the parent or legal guardian temporary rights to seek and provide healthcare and healthcare decisions on.
Web Updated June 03, 2022.
This additional information will assist in treatment if it can be furnished with the consent but is not required. Web it is understood that this authorization is given to provide authority and power on the part of my aforesaid agent(s) to give specific consent to any and all such evaluation, diagnosis, office treatment, anesthetic administration or surgical treatment(s) which a physician, in the exercise of his/her best judgment, may deem advisable. Web should your child need to be seen at nationwide children’s hospital, we must have your written consent to allow the person you select to seek treatment and sign the consent form. Web this consent form should be taken with the child to the hospital or physician's office when the child is taken for treatment.
Web This Consent Form Should Be Taken With The Child To The Hospital Or Physician's Office When The Child Is Taken For Treatment.
It is a simple one (1) page document that authorizes a third (3rd) party representative to handle any questions or requests by doctors or hospital staff in. I, (full name of parent or legal guardian) _____ A minor medical treatment authorization form allows a parent or guardian to select someone else to handle the primary health care decisions of their child. A copy of the authorization should be made a part of the minor's medical record.
Minors Under The Supervision Of Foster Parents:
This person must be 18 years of age or older. Web the simple form gives clear, irrefutable consent for medical treatment—until you can step in. Family address _____ father’s telephone: