Claim Form 1500 Pdf
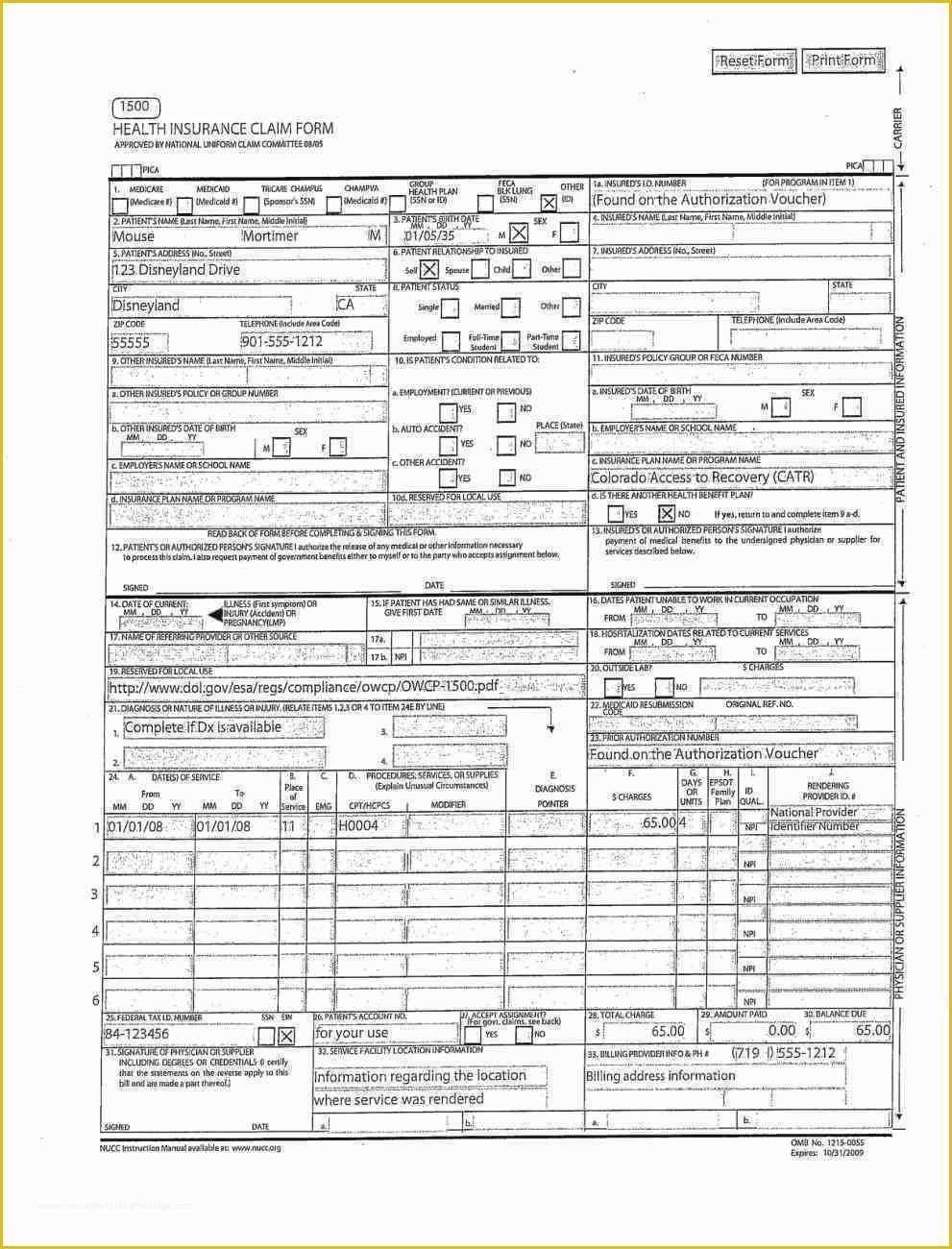
Claim Form 1500 Pdf - Download free cms 1500 claim form fillable template. Claims must be made within 12. Medicare medicaid champus champva other read back of form before completing & signing this form. Sign online button or tick the preview image of the blank. In the case of a medicare claim, the patient’s signature authorizes any entity to release to medicare medical and nonmedical information, including employment status, and whether the person has employer group health Insured’s name (last name, first name, middle initial). Read the instructions and tips below first. Number (for program in item 1) 4. The advanced tools of the editor will guide you through the editable pdf template. Web cms 1500 dynamic list information.
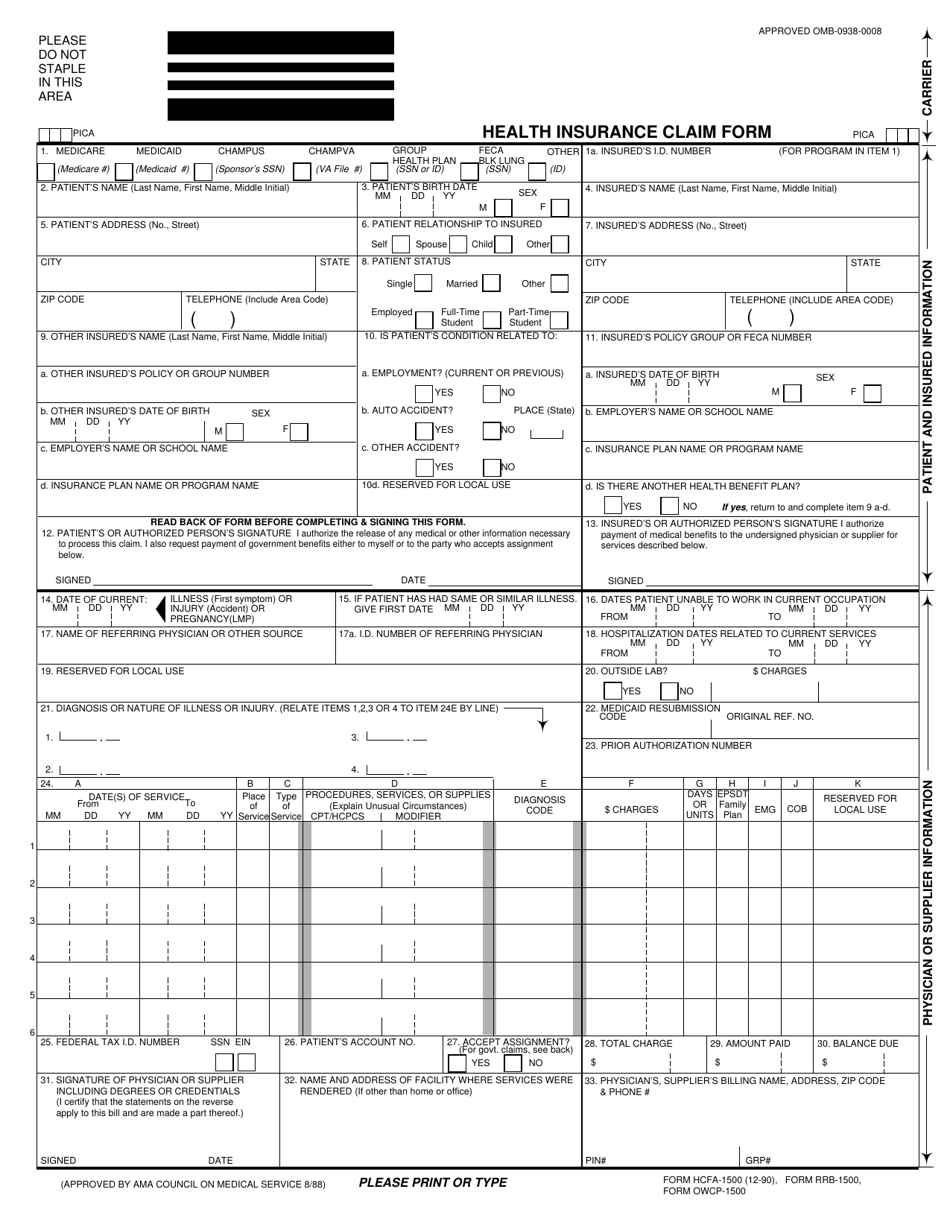
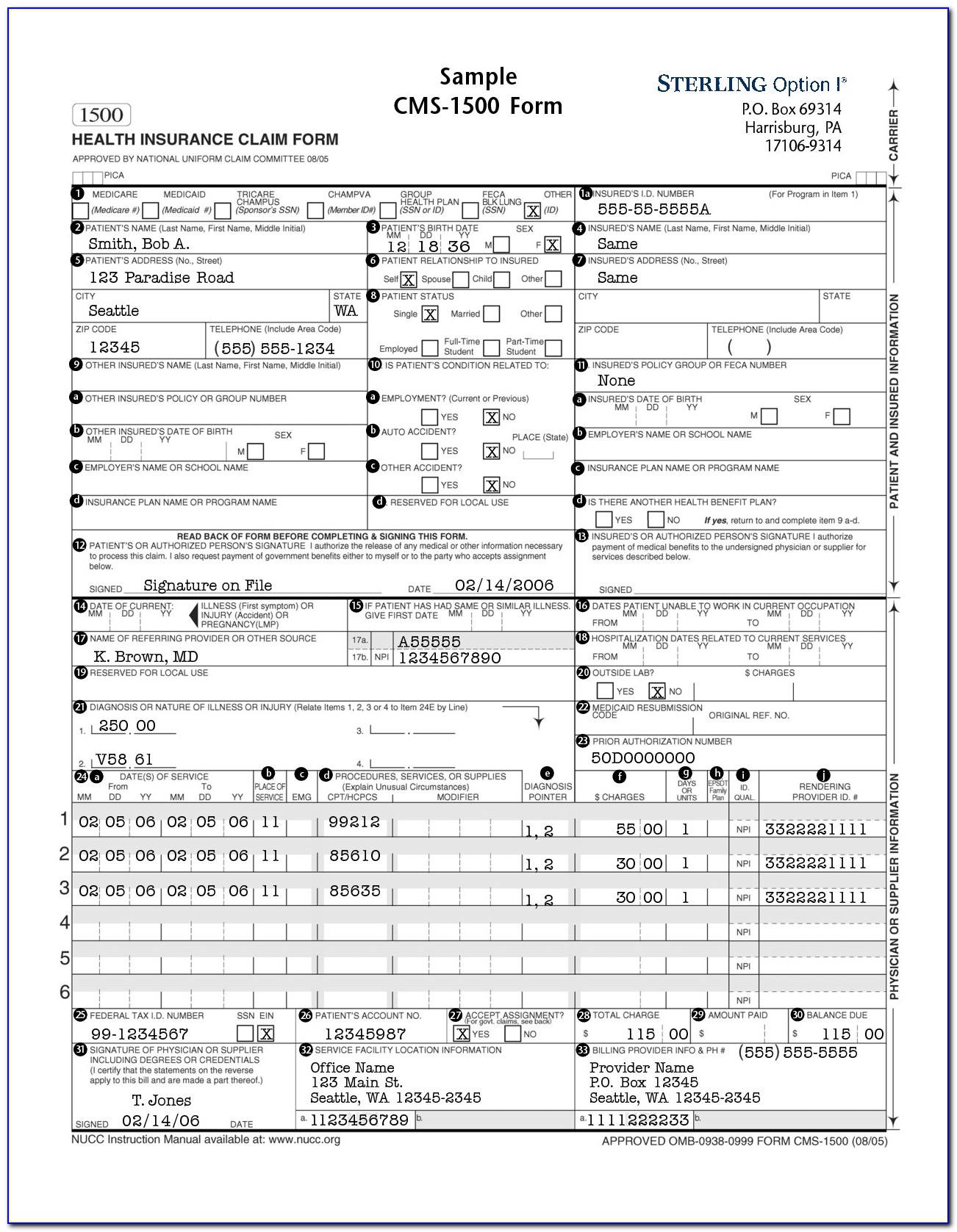
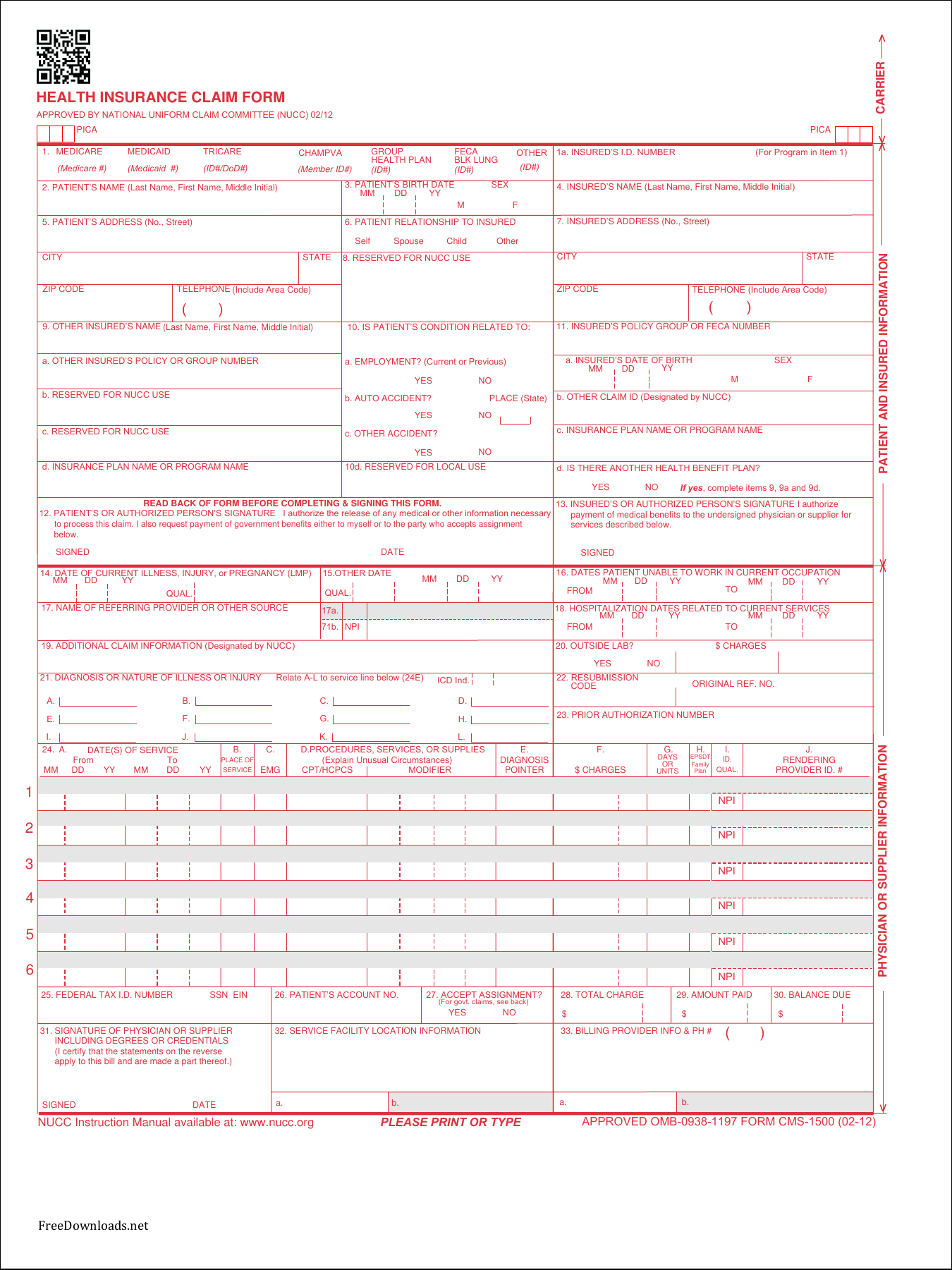
In addition to medicare parts a/b and for medicare durable medical equipment administrative contractors. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. Enter your official contact and identification details. Read the instructions and tips below first. The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. Download free cms 1500 claim form fillable template. Web download cms claim form 1500 which is used by health care professionals to bill medicare and medicaid. Number (for program in item 1) 4. Insured’s name (last name, first name, middle initial). Sign up to get the latest information about your choice of cms topics.
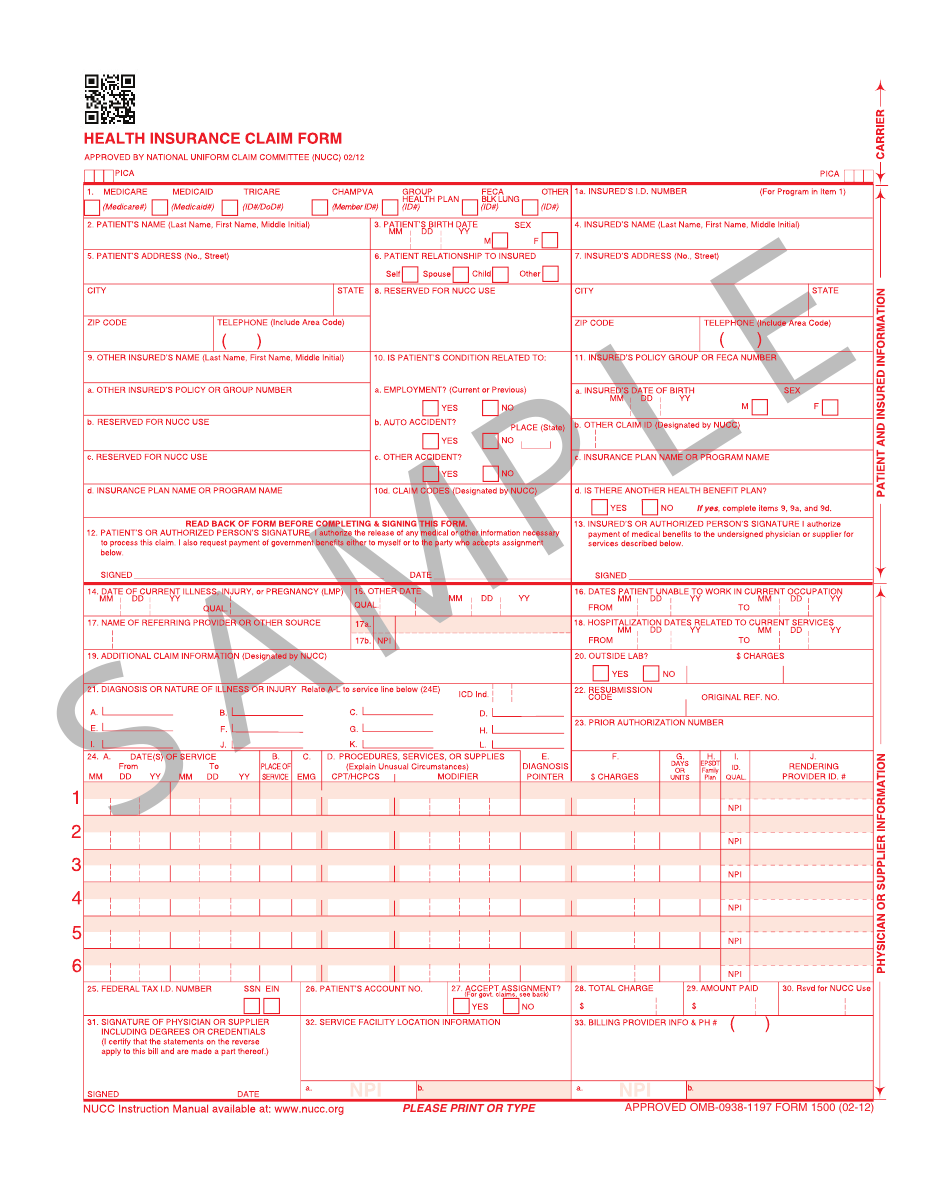
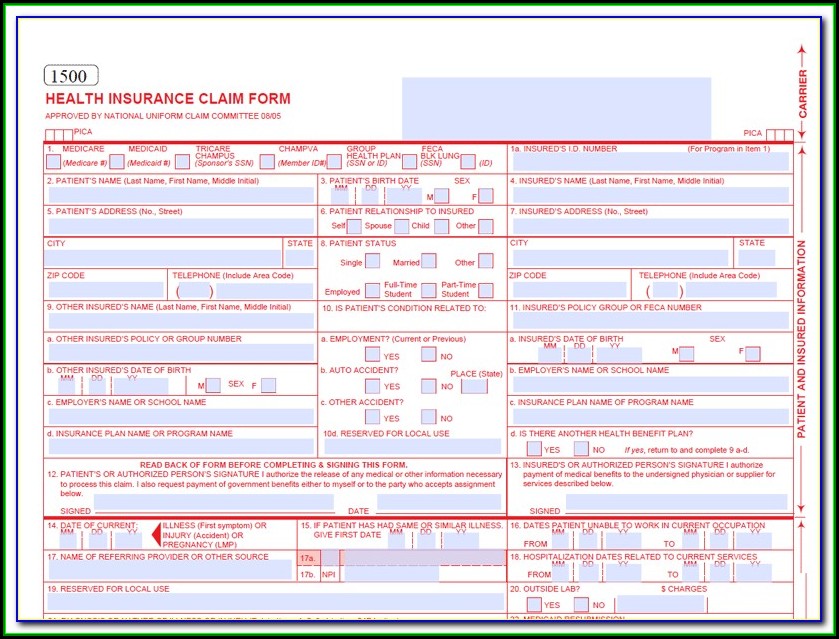
In the case of a medicare claim, the patient’s signature authorizes any entity to release to medicare medical and nonmedical information, including employment status, and whether the person has employer group health Web the claim and certifies that the information provided in blocks 1 through 12 is true, accurate and complete. Web health insurance claim form 1. Insured’s name (last name, first name, middle initial). In addition to medicare parts a/b and for medicare durable medical equipment administrative contractors. Web download cms claim form 1500 which is used by health care professionals to bill medicare and medicaid. Sign online button or tick the preview image of the blank. Health insurance claim form 1. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. The advanced tools of the editor will guide you through the editable pdf template.
Free Cms 1500 Claim form Template Of Hcfa 1500 Claim form Fillable Pdf
Medicare medicaid champus champva other read back of form before completing & signing this form. Web tips on how to fill out the hevalth claim form 1500 on the internet: Claims must be made within 12. To start the document, utilize the fill camp; Health insurance claim form 1.
Form HCFA1500 Download Printable PDF or Fill Online Health Insurance
Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. Read the instructions and tips below first. Web download pdf of cms 1500 claim form from the link available below in the article, cms 1500 claim form pdf free or read online using the direct link given at the bottom of content. Number (for.
Vidal Health Tpa Claim Form Pdf Form Resume Examples w950AzpOor
Download free cms 1500 claim form fillable template. Medicare medicaid champus champva other read back of form before completing & signing this form. You can decide how often to. Sign up to get the latest information about your choice of cms topics. Web the claim and certifies that the information provided in blocks 1 through 12 is true, accurate and.

Health Insurance Claim Form 1500 Download Form Resume Examples
Insured’s name (last name, first name, middle initial). The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. Read the instructions and tips below first. You can decide how often to. Web health insurance claim form 1.

cms1500claimformsample CASO Document Management
Medicare medicaid champus champva other read back of form before completing & signing this form. Number (for program in item 1) 4. Web download pdf of cms 1500 claim form from the link available below in the article, cms 1500 claim form pdf free or read online using the direct link given at the bottom of content. Medicare medicaid tricare.
Download Fillable CMS Claim Form 1500 PDF
Claims must be made within 12. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. Medicare medicaid tricare champva other read back of form before completing & signing this form. Web cms 1500 dynamic list information. Health insurance claim form 1.
Form 1500 Download Printable PDF or Fill Online Health Insurance Claim
Web download pdf of cms 1500 claim form from the link available below in the article, cms 1500 claim form pdf free or read online using the direct link given at the bottom of content. In the case of a medicare claim, the patient’s signature authorizes any entity to release to medicare medical and nonmedical information, including employment status, and.
Health Insurance Claim Form 1500 Fillable Pdf Free Form Resume
Web download cms claim form 1500 which is used by health care professionals to bill medicare and medicaid. You can decide how often to. Sign up to get the latest information about your choice of cms topics. Insured’s name (last name, first name, middle initial). Web cms 1500 dynamic list information.

Cms 1500 Claim Form Pdf Free Download Universal Network
To start the document, utilize the fill camp; Insured’s name (last name, first name, middle initial). Web download cms claim form 1500 which is used by health care professionals to bill medicare and medicaid. Sign online button or tick the preview image of the blank. Web download pdf of cms 1500 claim form from the link available below in the.
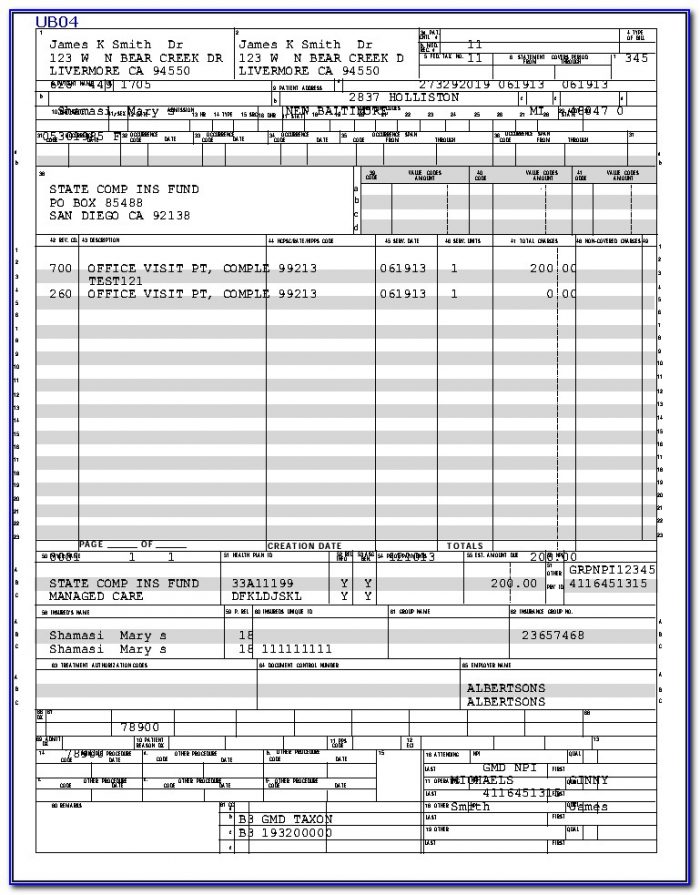
Ub 04 Form Printable Master of Documents
Web download pdf of cms 1500 claim form from the link available below in the article, cms 1500 claim form pdf free or read online using the direct link given at the bottom of content. Enter your official contact and identification details. Claims must be made within 12. In the case of a medicare claim, the patient’s signature authorizes any.
Claims Must Be Made Within 12.
Sign up to get the latest information about your choice of cms topics. Web the claim and certifies that the information provided in blocks 1 through 12 is true, accurate and complete. Read the instructions and tips below first. Insured’s name (last name, first name, middle initial).
Medicare Medicaid Tricare Champva Other Read Back Of Form Before Completing & Signing This Form.
Health insurance claim form 1. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. In addition to medicare parts a/b and for medicare durable medical equipment administrative contractors.
Enter Your Official Contact And Identification Details.
In the case of a medicare claim, the patient’s signature authorizes any entity to release to medicare medical and nonmedical information, including employment status, and whether the person has employer group health Web tips on how to fill out the hevalth claim form 1500 on the internet: To start the document, utilize the fill camp; Web cms 1500 dynamic list information.
You Can Decide How Often To.
Web health insurance claim form 1. Download free cms 1500 claim form fillable template. Sign online button or tick the preview image of the blank. Web download cms claim form 1500 which is used by health care professionals to bill medicare and medicaid.