Authorized Representative Form California
Authorized Representative Form California - I may not transfer or reassign my appointment. Web this form allows the ihss applicant/recipient or his/her legal representative to choose an authorized representative for the ihss program and identifies the functions the. Web authorized representative form keywords: Authorized representative form created date: The organization must give this signed and completed form to the county. Use black or blue ink. This form authorizes covered california to release. Privacy complaint form by a. Ealth and human services agency. C 382 (6/18) use this form to appoint an individual or.
To assign an authorized representative. Authorized representative form created date: Privacy complaint form by a. C 382 (6/18) use this form to appoint an individual or. You must completely fill out and sign the form, and mail it to: Web representative hbex 403 (07/17) authorization for release of personal information & appointment of representative. You (or your authorized representative) must complete part a of this form to let the county know who you. The organization must give this signed and completed form to the county. Web this form allows the ihss applicant/recipient or his/her legal representative to choose an authorized representative for the ihss program and identifies the functions the. Use black or blue ink.
Use black or blue ink. Web state of california. Web representative hbex 403 (07/17) authorization for release of personal information & appointment of representative. Web request to correct or dispute tax forms. Ealth and human services agency. Web authorized representative form you have the right to choose someone to represent you regarding your appeal or grievance with california health & wellness. This form authorizes covered california to release. Web this form allows the ihss applicant/recipient or his/her legal representative to choose an authorized representative for the ihss program and identifies the functions the. Appointment of authorized representative 1. Web use this form to authorize the franchise tax board (ftb) to release limited information for all taxable years to the authorized representative listed in part ii below.
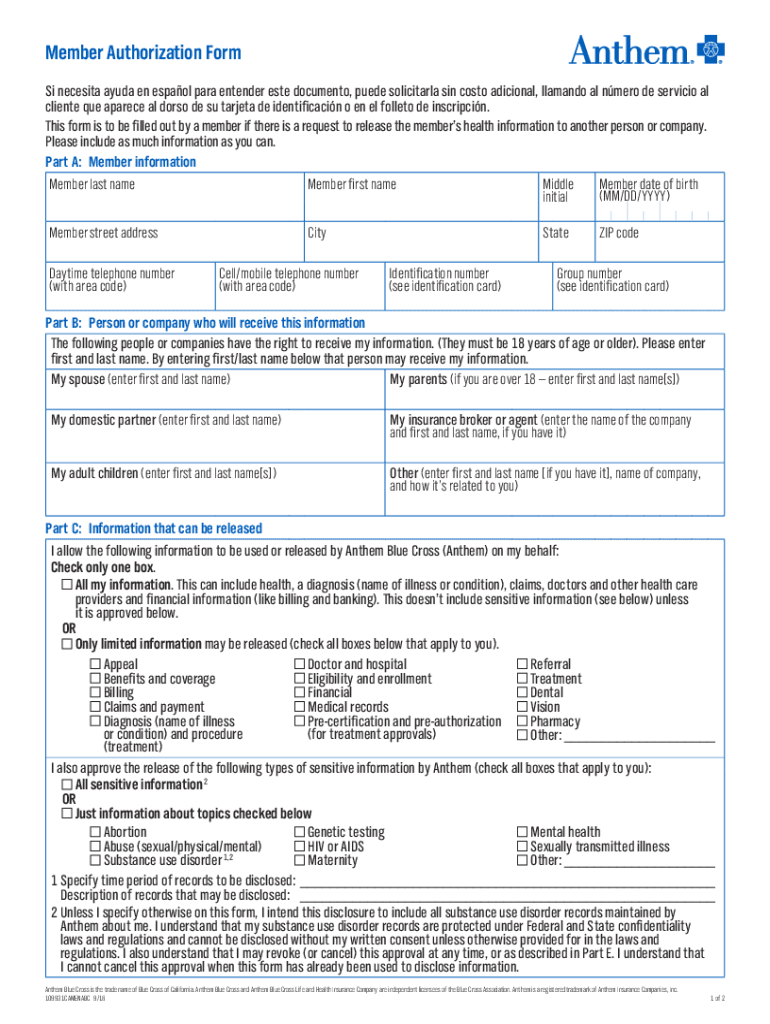
20182021 Anthem Member Authorization Form Fill Online, Printable
This form authorizes covered california to release. Privacy complaint form by a. Appointment of authorized representative 1. Web representative hbex 403 (07/17) authorization for release of personal information & appointment of representative. Web we created this site to provide useful information to individuals involved in our hearing process, including claimants, authorized representatives and county staff, and anyone.
Authorized Representative Instructions University Health Services
C 382 (6/18) use this form to appoint an individual or. Web state of california. You (or your authorized representative) must complete part a of this form to let the county know who you. Appointment of authorized representative 1. The organization must give this signed and completed form to the county.
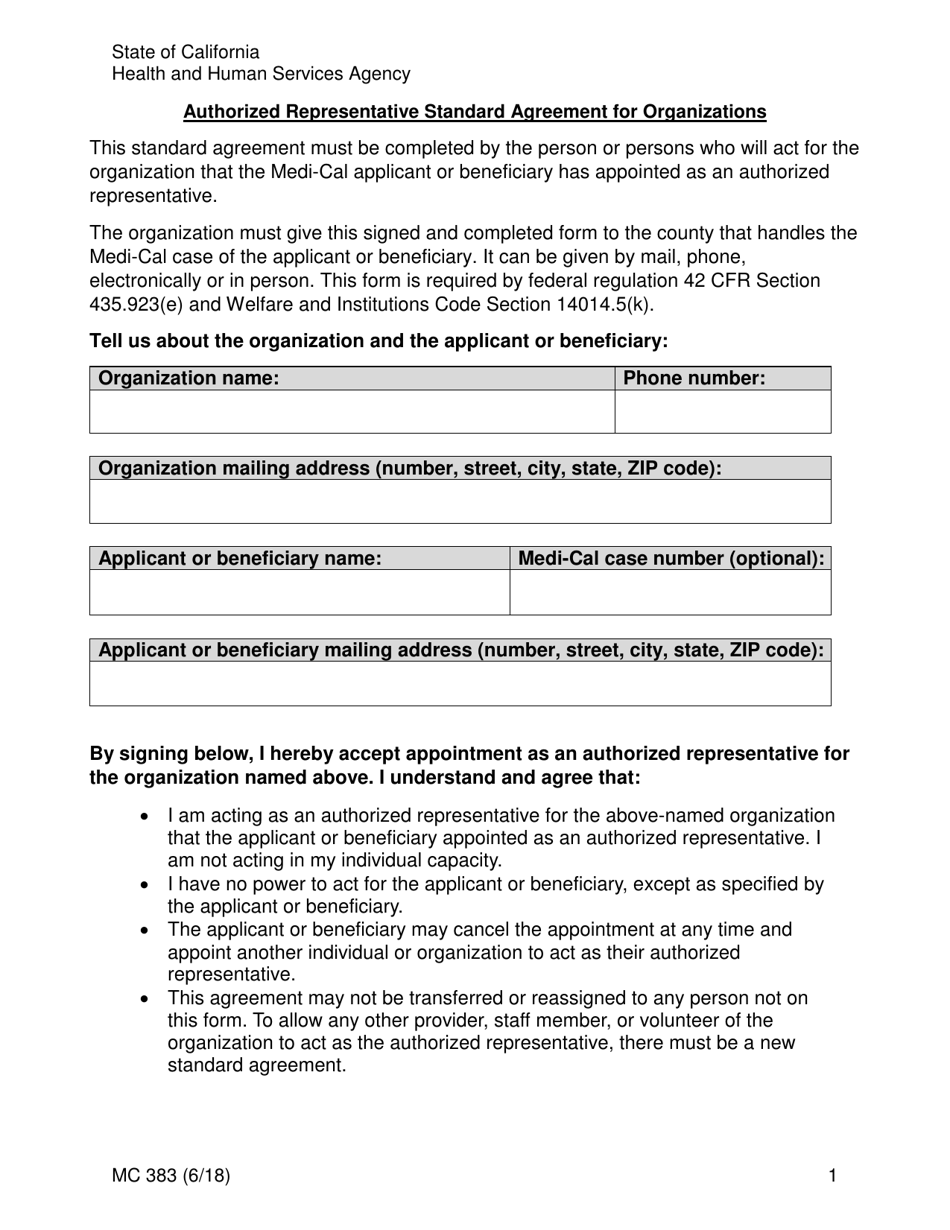
Form MC383 Download Fillable PDF or Fill Online Authorized
This form authorizes covered california to release. Appointment of authorized representative 1. Authorized representative form created date: C 382 (6/18) use this form to appoint an individual or. Web authorized representative form keywords:
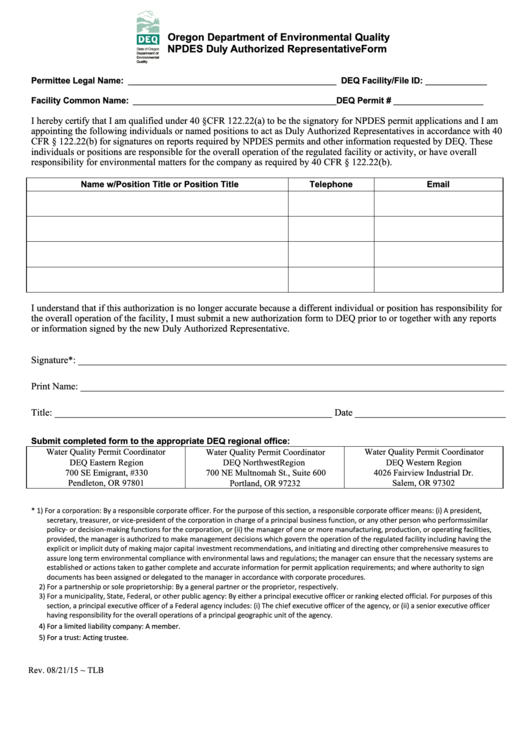
Fillable Duly Authorized Representative Form printable pdf download
The organization must give this signed and completed form to the county. Use black or blue ink. Web state of california. C 382 (6/18) use this form to appoint an individual or. I may not transfer or reassign my appointment.
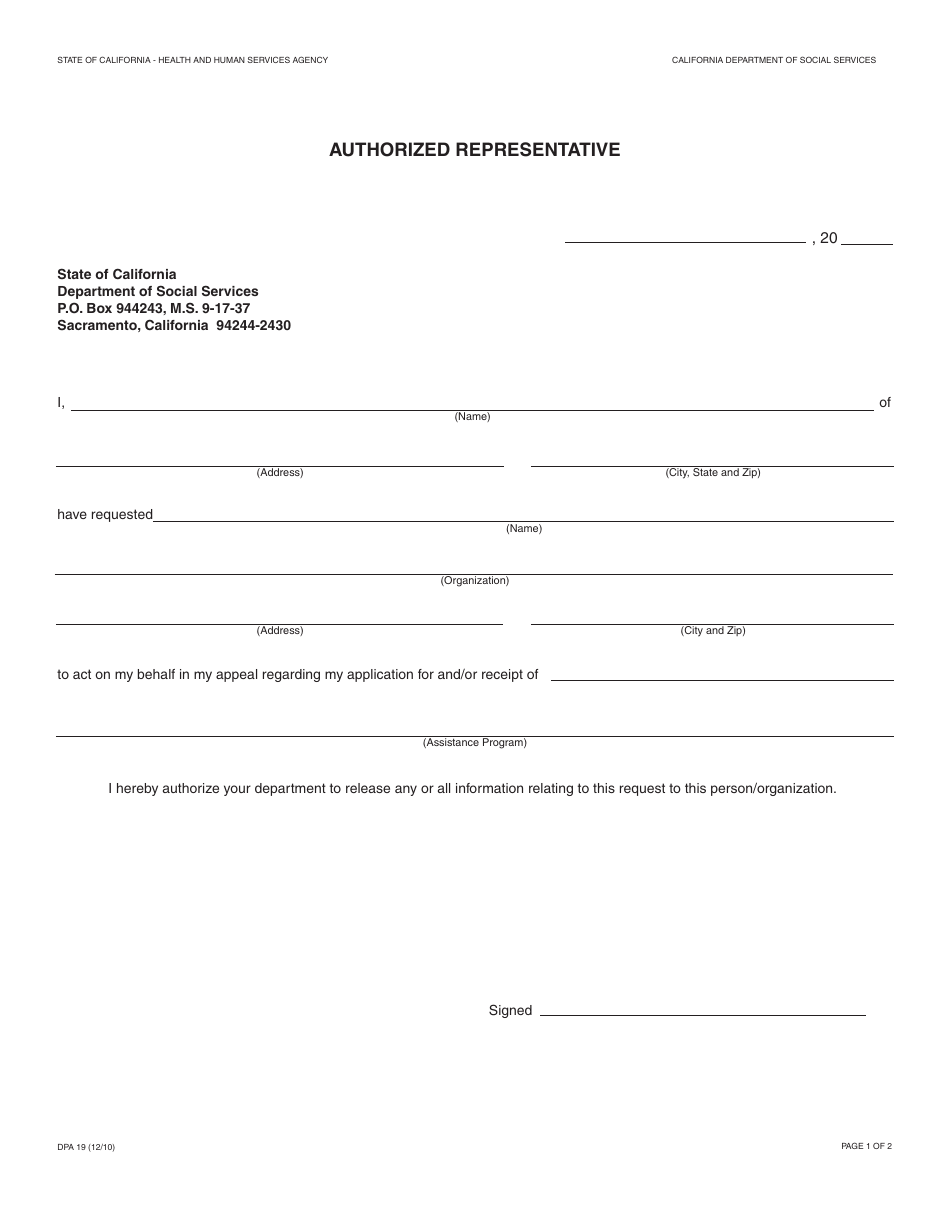
Form DPA19 Download Fillable PDF or Fill Online Authorized
The organization must give this signed and completed form to the county. Appointment of authorized representative 1. Web this form allows the ihss applicant/recipient or his/her legal representative to choose an authorized representative for the ihss program and identifies the functions the. I may not transfer or reassign my appointment. You (or your authorized representative) must complete part a of.
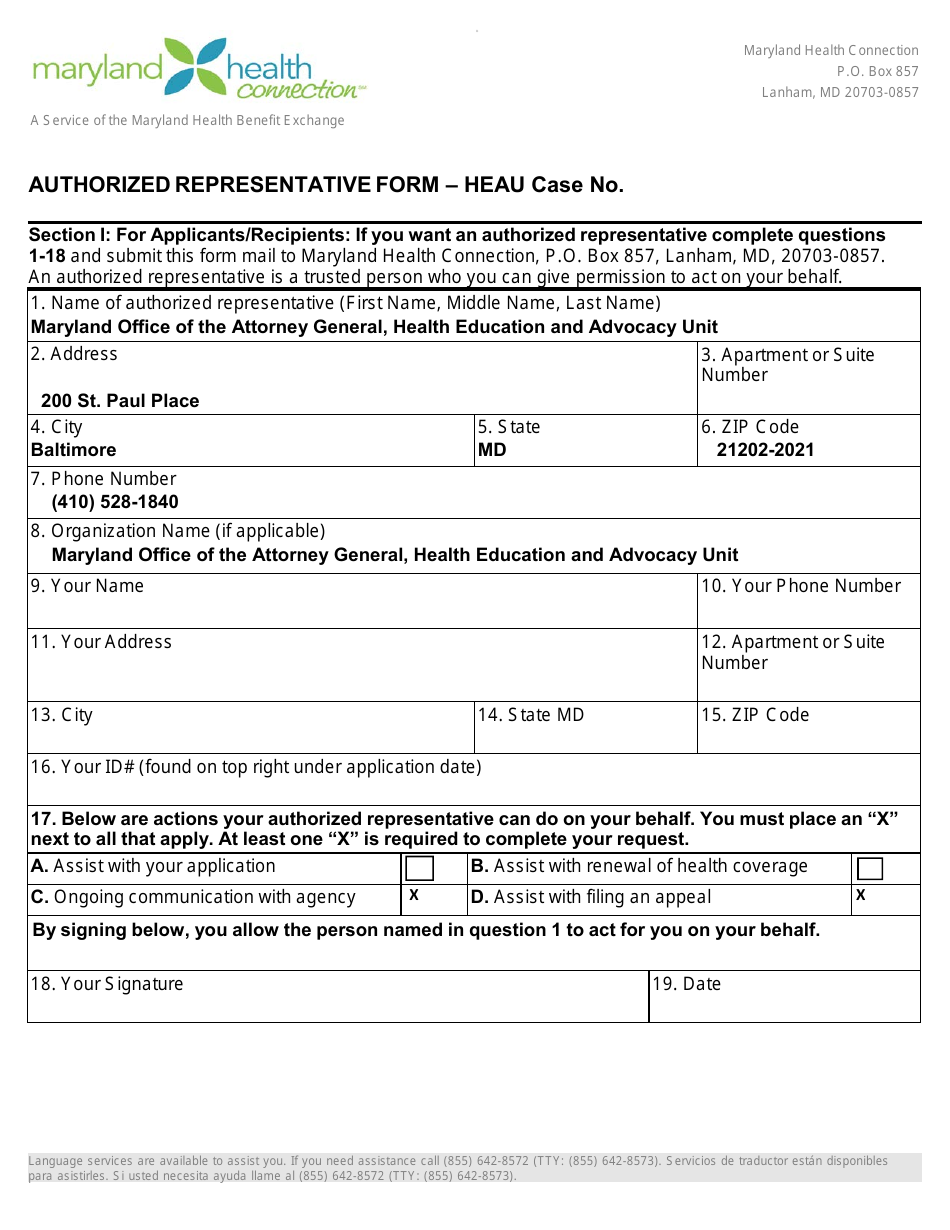
Maryland Authorized Representative Form Heau Download Fillable PDF
Use black or blue ink. Ealth and human services agency. Appointment of authorized representative 1. I may not transfer or reassign my appointment. Web state of california.
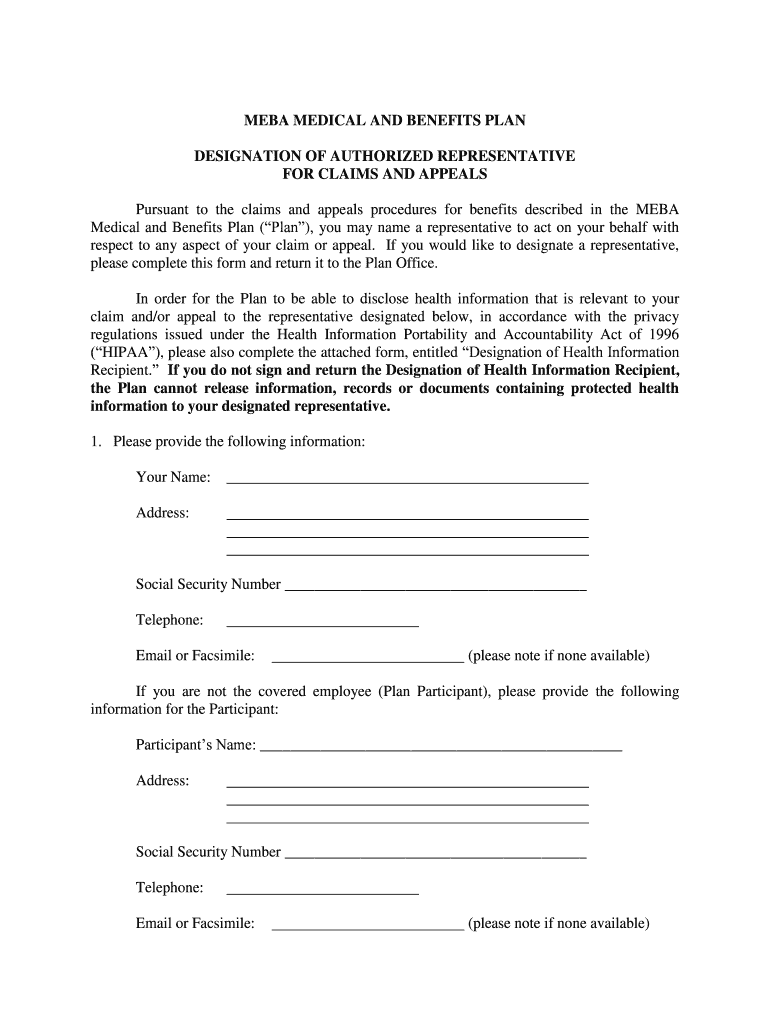
MEBA Medical Plan Designation of Authorized Representative Form Fill
C 382 (6/18) use this form to appoint an individual or. Ealth and human services agency. Appointment of authorized representative 1. Web authorized representative form you have the right to choose someone to represent you regarding your appeal or grievance with california health & wellness. The organization must give this signed and completed form to the county.

Alameda Alliance Prior Authorization Form Pdf Fill Online, Printable
Web this form allows the ihss applicant/recipient or his/her legal representative to choose an authorized representative for the ihss program and identifies the functions the. Web use this form to authorize the franchise tax board (ftb) to release limited information for all taxable years to the authorized representative listed in part ii below. Web authorized representative form keywords: This form.
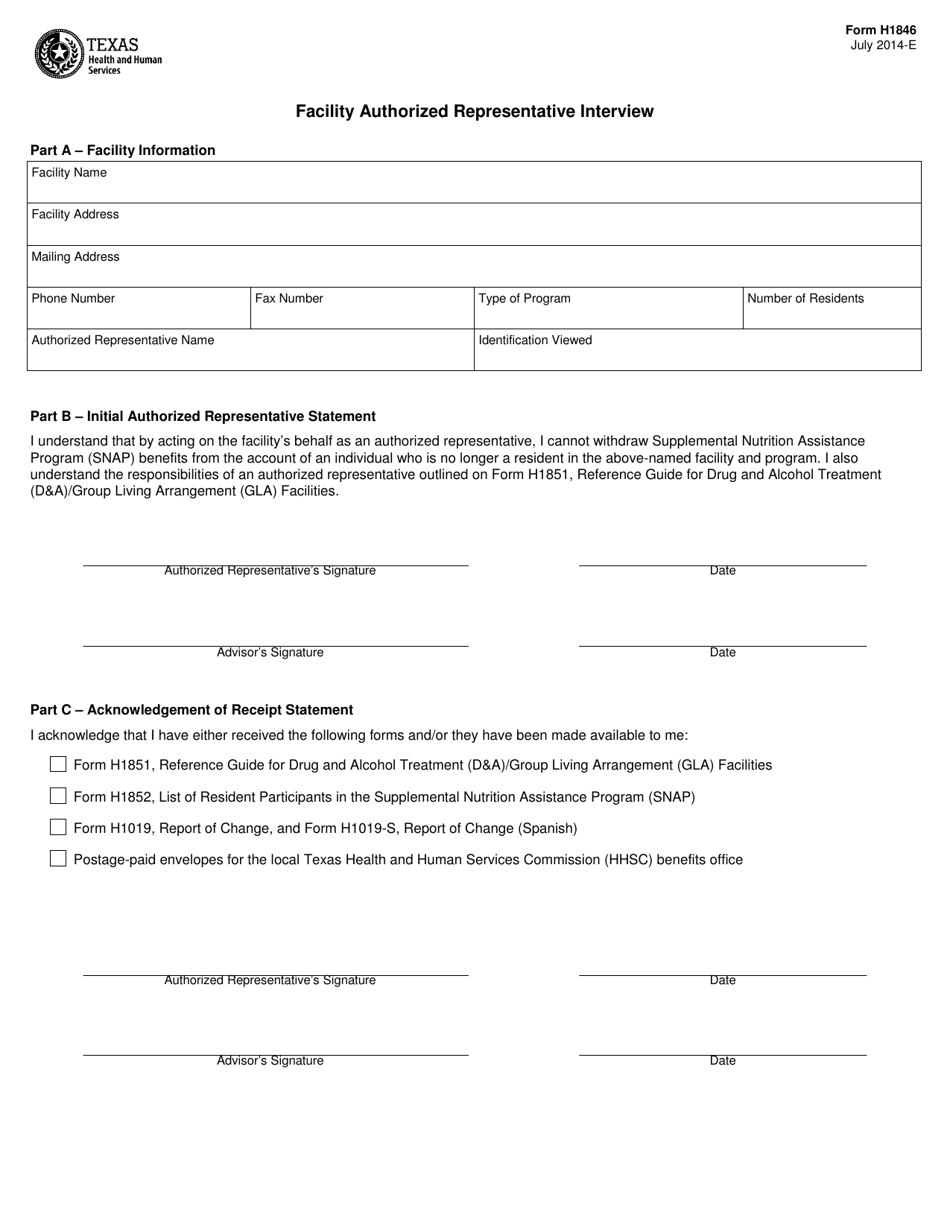
Form H1846 Download Printable PDF or Fill Online Facility Authorized
Privacy complaint form by a. Web representative hbex 403 (07/17) authorization for release of personal information & appointment of representative. Web authorized representative form keywords: Authorized representative form created date: Ealth and human services agency.

Authorized Representative Form Sample Fill and Sign Printable
Web representative hbex 403 (07/17) authorization for release of personal information & appointment of representative. Privacy complaint form by a. Authorized representative form created date: Appointment of authorized representative 1. Web state of california.
Web Use This Form To Authorize The Franchise Tax Board (Ftb) To Release Limited Information For All Taxable Years To The Authorized Representative Listed In Part Ii Below.
Appointment of authorized representative 1. C 382 (6/18) use this form to appoint an individual or. Web we created this site to provide useful information to individuals involved in our hearing process, including claimants, authorized representatives and county staff, and anyone. You (or your authorized representative) must complete part a of this form to let the county know who you.
Web Authorized Representative Form Keywords:
The organization must give this signed and completed form to the county. Web request to correct or dispute tax forms. To assign an authorized representative. Authorized representative form created date:
Use Black Or Blue Ink.
Web representative hbex 403 (07/17) authorization for release of personal information & appointment of representative. Web state of california. Web this form allows the ihss applicant/recipient or his/her legal representative to choose an authorized representative for the ihss program and identifies the functions the. Web authorized representative form you have the right to choose someone to represent you regarding your appeal or grievance with california health & wellness.
Ealth And Human Services Agency.
Privacy complaint form by a. This form authorizes covered california to release. I may not transfer or reassign my appointment. You must completely fill out and sign the form, and mail it to: