Ambetter Appeal Form Texas
Ambetter Appeal Form Texas - If you have questions about the. You must file an appeal within 180 days of the date on the denial letter. Biopharmacy outpatient prior authorization form (j. Provider disputes po box 9040. Ambetter from arizona complete health attn: Web you will need adobe reader to open pdfs on this site. Select your state to contact an ambetter representative in your service area. Web español if you disagree with a decision made by your health plan, you have several options. Easily fill out pdf blank, edit, and sign them. Web complete ambetter reconsideration form texas online with us legal forms.
Web appeal you file an appeal in response to a denial received from ambetter from health net. Web a claim dispute/claim appeal must be submitted on this claim dispute/appeal form, which can also be found on our website. All fields are required information a request for. Web • ambetter will acknowledge receipt within 10 business days of receiving the appeal. You must file an appeal within 180 days of the date on the denial letter. Read below to find out how to appeal a decision, file a complaint, and ask for an external. Web if you have questions or concerns about your health insurance coverage, we'd love to hear from you. Select your state to contact an ambetter representative in your service area. Provider disputes po box 9040. Use your zip code to find your personal plan.
Web complete ambetter reconsideration form texas online with us legal forms. Web • ambetter will acknowledge receipt within 10 business days of receiving the appeal. Ambetter from arizona complete health attn: Web fax authorization request primary procedure code* additional procedure code start date or admission date * diagnosis code * (cpt/hcpcs) (modifier). Web a claim dispute/claim appeal must be submitted on this claim dispute/appeal form, which can also be found on our website. Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. Web appeal by phone, fax, or in person. All fields are required information a request for. If you have questions about the. The completed form can be returned by mail or fax.
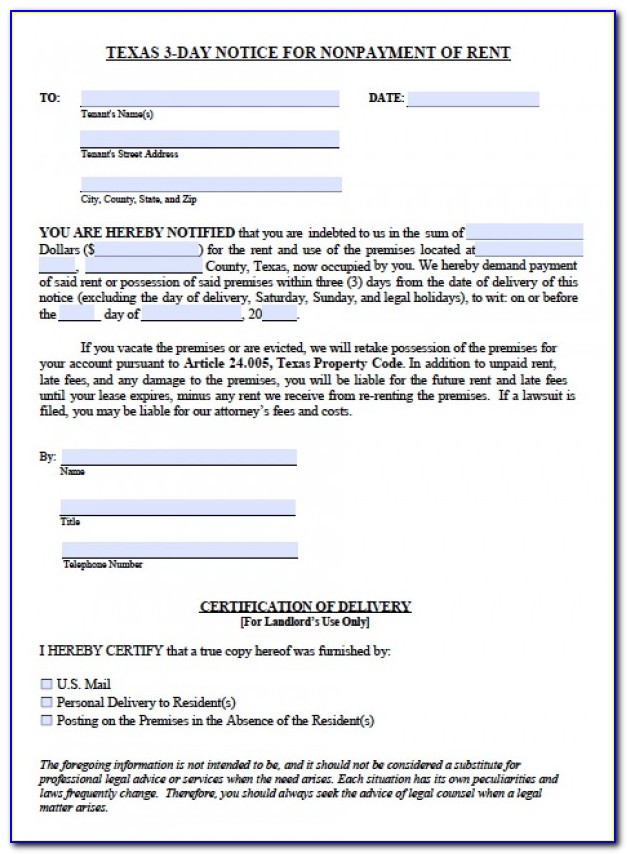
3 Day Eviction Notice California Form
Web • ambetter will acknowledge receipt within 10 business days of receiving the appeal. Web español if you disagree with a decision made by your health plan, you have several options. Complex imaging, mra, mri, pet, and ct scans, as well as speech, occupational and physical. Web you, your provider, a friend, a relative, lawyer or another spokesperson can request.

Ambetter Prior Authorization form Awesome Lookasserta Urlscan
Web inpatient prior authorization fax form (pdf) outpatient prior authorization fax form (pdf) grievance and appeals; Web • ambetter will acknowledge receipt within 10 business days of receiving the appeal. If you have questions about the. Biopharmacy outpatient prior authorization form (j. All fields are required information a request for.

ambetter secure care 20 darlenaohlemacher
Web español if you disagree with a decision made by your health plan, you have several options. The completed form can be returned by mail or fax. Web you will need adobe reader to open pdfs on this site. You must file an appeal within 180 days of the date on the denial letter. Web if you have questions or.
Ambetter Insurance Providers Texas / Ambetter From Coordinated Care
Web the panel will make a recommendation for the final decision on the member complaint, and ambetter’s final decision will be provided to the member within thirty (30) days of the. Biopharmacy outpatient prior authorization form (j. • ambetter will resolve each appeal and provide written notice as expeditiously as the. If you have questions about the. You must file.

What Is The Group Id For Ambetter / Where can I find the policy number
Web the panel will make a recommendation for the final decision on the member complaint, and ambetter’s final decision will be provided to the member within thirty (30) days of the. Ambetter from arizona complete health attn: Read below to find out how to appeal a decision, file a complaint, and ask for an external. Mail completed form(s) and attachments.

Consumer Debt Litigation (mostly Texas) Appealing Pro Se in Texas
Complex imaging, mra, mri, pet, and ct scans, as well as speech, occupational and physical. Mail completed form(s) and attachments to the appropriate address: Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. Web find our member handbooks, forms, and resources all in one place! Web fax authorization request primary procedure.

Ambetter Prior Authorization form Brilliant Envision Rx Prior
Web forms claims claims appeal (pdf) claims reconsideration (pdf) cms1500 (pdf) corrected claim (pdf) request for claim status (pdf) ub04 (pdf) member. Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. If you have questions about the. Web • ambetter will acknowledge receipt within 10 business days of receiving the appeal..

Texas Notice Of Appeal Form Fill Online, Printable, Fillable, Blank
Web fax authorization request primary procedure code* additional procedure code start date or admission date * diagnosis code * (cpt/hcpcs) (modifier). Web inpatient prior authorization fax form (pdf) outpatient prior authorization fax form (pdf) grievance and appeals; Provider disputes po box 9040. Web complete ambetter reconsideration form texas online with us legal forms. All fields are required information a request.
What Is The Group Id For Ambetter Ambetter Insurance Card Images
Biopharmacy outpatient prior authorization form (j. Easily fill out pdf blank, edit, and sign them. Complex imaging, mra, mri, pet, and ct scans, as well as speech, occupational and physical. Web appeal by phone, fax, or in person. Web a claim dispute/claim appeal must be submitted on this claim dispute/appeal form, which can also be found on our website.

Ambetter Insurance Texas Providers Ambetter Superior Health Plan
Web find our member handbooks, forms, and resources all in one place! Web español if you disagree with a decision made by your health plan, you have several options. Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. You must file an appeal within 180 days of the date on the.
Biopharmacy Outpatient Prior Authorization Form (J.
Select your state to contact an ambetter representative in your service area. Web find our member handbooks, forms, and resources all in one place! Mail completed form(s) and attachments to the appropriate address: Ambetter from arizona complete health attn:
Web A Claim Dispute/Claim Appeal Must Be Submitted On This Claim Dispute/Appeal Form, Which Can Also Be Found On Our Website.
Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. Access the find a provider guide, member handbook, and reimbursement forms. Web use this form as part of the ambetter from coordinated care request for reconsideration and claim dispute process. Web inpatient prior authorization fax form (pdf) outpatient prior authorization fax form (pdf) grievance and appeals;
The Completed Form Can Be Returned By Mail Or Fax.
The claim dispute form must be completed in its. Web español if you disagree with a decision made by your health plan, you have several options. Web appeal by phone, fax, or in person. Complex imaging, mra, mri, pet, and ct scans, as well as speech, occupational and physical.
Web The Panel Will Make A Recommendation For The Final Decision On The Member Complaint, And Ambetter’s Final Decision Will Be Provided To The Member Within Thirty (30) Days Of The.
Save or instantly send your ready documents. Web • ambetter will acknowledge receipt within 10 business days of receiving the appeal. Web if you have questions or concerns about your health insurance coverage, we'd love to hear from you. Web fax authorization request primary procedure code* additional procedure code start date or admission date * diagnosis code * (cpt/hcpcs) (modifier).