Aarp Appeal Form
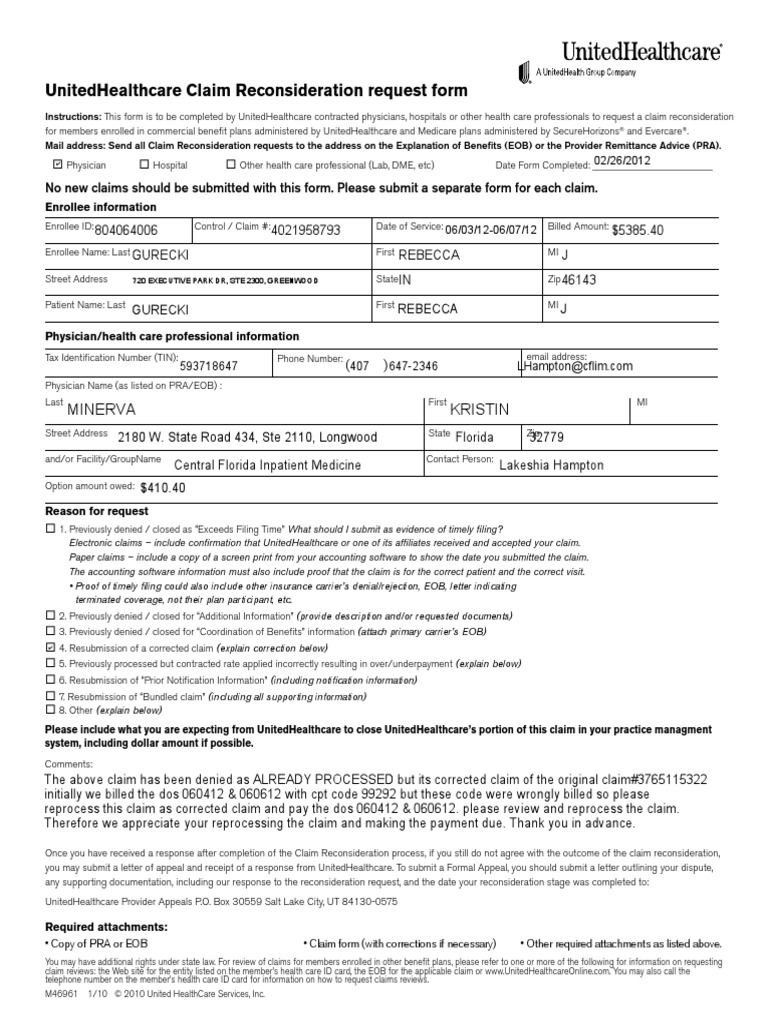
Aarp Appeal Form - Mail or fax the letter or completed form to unitedhealthcare. Web single claim reconsideration/corrected claim request form this form is to be completed by physicians, hospitals or other health care professionals for claim reconsideration requests for our members. Web you may file an appeal within sixty (60) calendar days of the date of the notice of the initial organization determination. One man's obsession with cracking cold cases. Web how age bias helped a killer continue his spree. For example, you may file an appeal for any of the following reasons: • please submit a separate form for each claim • no new claims should be submitted with this form Loving families or elder abuse? Web get your online template and fill it in using progressive features. Web how do i file an appeal for my claim?
Web write a letter describing your appeal or use the redetermination request form (pdf) (67.62 kb). Web you may file an appeal within sixty (60) calendar days of the date of the notice of the initial organization determination. Finding a legal specialist, making an appointment and going to the business office for a private conference makes completing a aarp provider appeal form from beginning to end stressful. A shocking tale of love and abuse allegations. For example, you may file an appeal for any of the following reasons: Give your 'verdict' in these real court cases. Enjoy smart fillable fields and interactivity. Loving families or elder abuse? Web how age bias helped a killer continue his spree. Your medicare advantage health plan refuses to cover or pay for items/services or a part b drug you think your medicare advantage health plan should.
Finding a legal specialist, making an appointment and going to the business office for a private conference makes completing a aarp provider appeal form from beginning to end stressful. The last page of your notice lists the date that the. A shocking tale of love and abuse allegations. Enjoy smart fillable fields and interactivity. Mail or fax the letter or completed form to unitedhealthcare. • please submit a separate form for each claim • no new claims should be submitted with this form Web how age bias helped a killer continue his spree. For example, you may file an appeal for any of the following reasons: Web write a letter describing your appeal or use the redetermination request form (pdf) (67.62 kb). Your medicare advantage health plan refuses to cover or pay for items/services or a part b drug you think your medicare advantage health plan should.
Uhc Appeal Form for Corrected Claim Health Care Public Health
Web how do i file an appeal for my claim? His drawings help families identify missing persons. The last page of your notice lists the date that the. If you still disagree with the claim decision as an original medicare beneficiary, you have 120 days after receiving the msn to file an appeal. Your medicare advantage health plan refuses to.
Aarp Overpayment Refund Form Form Resume Examples e79Q5lx9kQ
Web how age bias helped a killer continue his spree. Web write a letter describing your appeal or use the redetermination request form (pdf) (67.62 kb). Choose the get form button to open it and begin editing. His drawings help families identify missing persons. Fill out all the required fields (they will be yellowish).
Optumrx Prior Authorization Form Cialis Rx Prior Authorization
Web how age bias helped a killer continue his spree. The last days of stan lee. Web you may file an appeal within sixty (60) calendar days of the date of the notice of the initial organization determination. A shocking tale of love and abuse allegations. Enjoy smart fillable fields and interactivity.
Aarp Provider Enrollment Form Form Resume Examples xg5bQljDlY
Choose the get form button to open it and begin editing. Web get your online template and fill it in using progressive features. Finding a legal specialist, making an appointment and going to the business office for a private conference makes completing a aarp provider appeal form from beginning to end stressful. Web how age bias helped a killer continue.

Delta Dental Provider Dispute Form Pdf FORM.UDLVIRTUAL.EDU.PE
Wolff, kimberly a created date: One man's obsession with cracking cold cases. Choose the template you want in the collection of legal forms. Web get your online template and fill it in using progressive features. Follow the simple instructions below:
Prior Authorization Request Form Fill Online, Printable, Fillable
Choose the template you want in the collection of legal forms. The last days of stan lee. His drawings help families identify missing persons. Mail or fax the letter or completed form to unitedhealthcare. Give your 'verdict' in these real court cases.

Prior Authorization Form For Aarp Medicare Complete Universal Network
Enjoy smart fillable fields and interactivity. Web how age bias helped a killer continue his spree. Web execute aarp appeal form in several minutes by using the guidelines listed below: The last page of your notice lists the date that the. Web how do i file an appeal for my claim?

Consumer Cellular Aarp Coverage Map Map Resume Examples Rg8DAby1Mq
Wolff, kimberly a created date: Enjoy smart fillable fields and interactivity. Give your 'verdict' in these real court cases. For example, you may file an appeal for any of the following reasons: Web write a letter describing your appeal or use the redetermination request form (pdf) (67.62 kb).

Aarp Medicare Part B Prior Authorization Form Form Resume Examples
His drawings help families identify missing persons. Www.uhcmedicaresolutions.com expedited appeal requests can be made by phone at: Web how age bias helped a killer continue his spree. The last page of your notice lists the date that the. Web how do i file an appeal for my claim?
Aarp Printable Application Pdf Fill Online, Printable, Fillable
Wolff, kimberly a created date: Web execute aarp appeal form in several minutes by using the guidelines listed below: For example, you may file an appeal for any of the following reasons: Web you may file an appeal within sixty (60) calendar days of the date of the notice of the initial organization determination. Loving families or elder abuse?
His Drawings Help Families Identify Missing Persons.
Web you may file an appeal within sixty (60) calendar days of the date of the notice of the initial organization determination. Finding a legal specialist, making an appointment and going to the business office for a private conference makes completing a aarp provider appeal form from beginning to end stressful. • please submit a separate form for each claim • no new claims should be submitted with this form Choose the get form button to open it and begin editing.
Choose The Template You Want In The Collection Of Legal Forms.
Www.uhcmedicaresolutions.com expedited appeal requests can be made by phone at: Mail or fax the letter or completed form to unitedhealthcare. Web how age bias helped a killer continue his spree. Web execute aarp appeal form in several minutes by using the guidelines listed below:
Web Write A Letter Describing Your Appeal Or Use The Redetermination Request Form (Pdf) (67.62 Kb).
Your medicare advantage health plan refuses to cover or pay for items/services or a part b drug you think your medicare advantage health plan should. Web get your online template and fill it in using progressive features. For example, you may file an appeal for any of the following reasons: Web you may also ask us for an appeal through our website at:
Give Your 'Verdict' In These Real Court Cases.
Web single claim reconsideration/corrected claim request form this form is to be completed by physicians, hospitals or other health care professionals for claim reconsideration requests for our members. Enjoy smart fillable fields and interactivity. Fill out all the required fields (they will be yellowish). One man's obsession with cracking cold cases.